

Phenotypic diversity in white adults with moderate to severe Class II malocclusion
- PMID: 24582022
- PMCID: PMC4007218
- DOI: 10.1016/j.ajodo.2013.11.013
Phenotypic diversity in white adults with moderate to severe Class II malocclusion
Abstract
Introduction: Class II malocclusion affects about 15% of the population in the United States and is characterized by a convex profile and occlusal disharmonies. The specific etiologic mechanisms resulting in the range of Class II dentoskeletal combinations observed are not yet understood. Most studies describing Class II phenotypic diversity have used moderate sample sizes or focused on younger patients who later in life might outgrow their Class II discrepancies; such a focus might also preclude the visualization of adult Class II features. The majority have used simple correlation methods resulting in phenotypes that might not be generalizable to different samples and thus might not be suitable for studies of malocclusion etiology. The purpose of this study was to address these knowledge gaps by capturing the maximum phenotypic variations in a large sample of white Class II subjects selected with strict eligibility criteria and rigorously standardized multivariate reduction analyses.
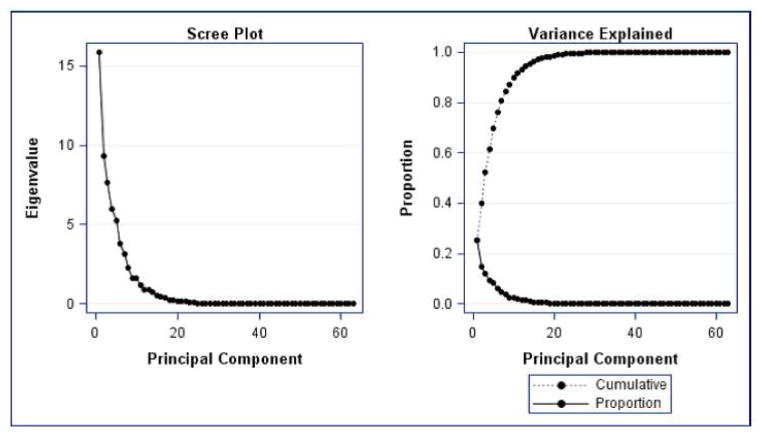
Methods: Sixty-three lateral cephalometric variables were measured from the pretreatment records of 309 white Class II adults (82 male, 227 female; ages, 16-60 years). Principal component analysis and cluster analysis were used to generate comprehensive phenotypes to identify the most homogeneous groups of subjects, reducing heterogeneity and improving the power of future malocclusion etiology studies.
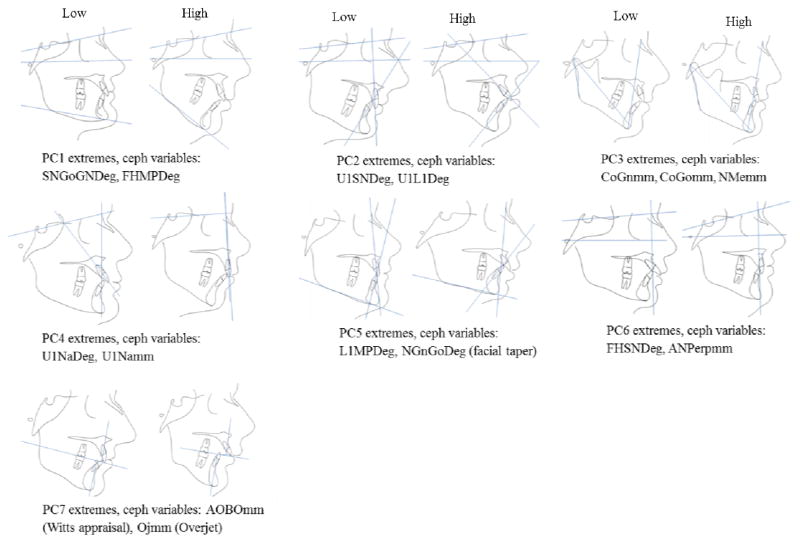
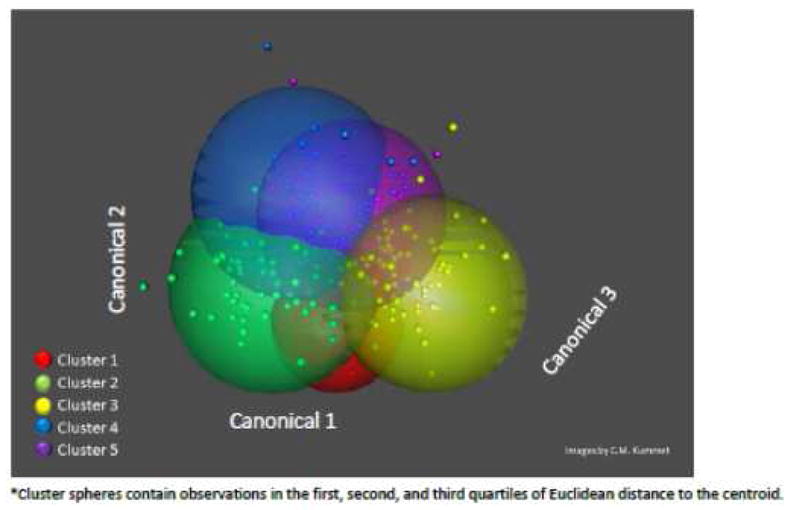
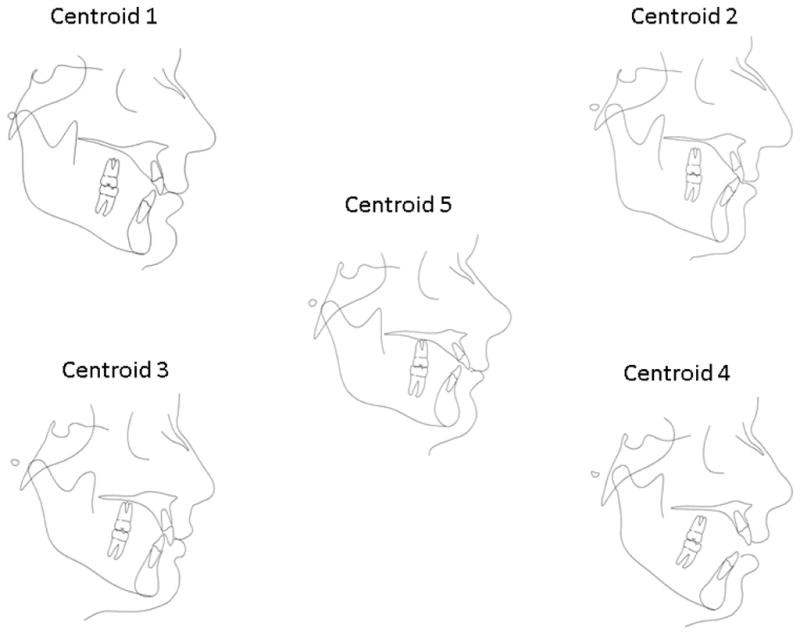
Results: Principal component analysis resulted in 7 principal components that accounted for 81% of the variation. The first 3 components represented variation on mandibular rotation, maxillary incisor angulation, and mandibular length. The cluster analysis identified 5 distinct Class II phenotypes.
Conclusions: A comprehensive spectrum of Class II phenotypic definitions was obtained that can be generalized to other samples to advance our efforts for identifying the etiologic factors underlying Class II malocclusion.
Copyright © 2014 American Association of Orthodontists. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Proffit WR, Fields HW, Sarver DM. In: Contemporary Orthodontics. 4. Proffit William R, Fields Henry W, Jr, Sarver David M., editors. St. Louis, Mo: Mosby Elsevier; 2007.
-
- Sant’Anna LB, Tosello DO. Fetal alcohol syndrome and developing craniofacial and dental structures--a review. Orthod Craniofac Res. 2006;9:172–185. - PubMed
-
- Naidoo S, Harris A, Swanevelder S, Lombard C. Foetal alcohol syndrome: a cephalometric analysis of patients and controls. Eur J Orthod. 2006;28:254–261. - PubMed
-
- Rythen M, Thilander B, Robertson A. Dento-alveolar characteristics in adolescents born extremely preterm. Eur J Orthod. 2012 - PubMed
-
- Warren JJ, Slayton RL, Bishara SE, Levy SM, Yonezu T, Kanellis MJ. Effects of nonnutritive sucking habits on occlusal characteristics in the mixed dentition. Pediatr Dent. 2005;27:445–450. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
