

Benchmarks for operative outcomes of robotic and open radical prostatectomy: results from the Health Professionals Follow-up Study
- PMID: 24582327
- PMCID: PMC4128909
- DOI: 10.1016/j.eururo.2014.01.039
Benchmarks for operative outcomes of robotic and open radical prostatectomy: results from the Health Professionals Follow-up Study
Abstract
Background: Robot-assisted laparoscopic radical prostatectomy (RALP) has become increasingly common; however, there have been no nationwide, population-based, non-claims-based studies to evaluate differences in outcomes between RALP and open radical retropubic prostatectomy (RRP).
Objective: To determine surgical, oncologic, and health-related quality of life (HRQOL) outcomes following RALP and RRP in a nationwide cohort.
Design, setting, and participants: We identified 903 men in the Health Professionals Follow-up Study diagnosed with prostate cancer between 2000 and 2010 who underwent radical prostatectomy using RALP (n=282) or RRP (n=621) as primary treatment.
Intervention: Radical prostatectomy.
Outcome measurements and statistical analysis: We compared patients undergoing RALP or RRP across a range of perioperative, oncologic, and HRQOL outcomes.
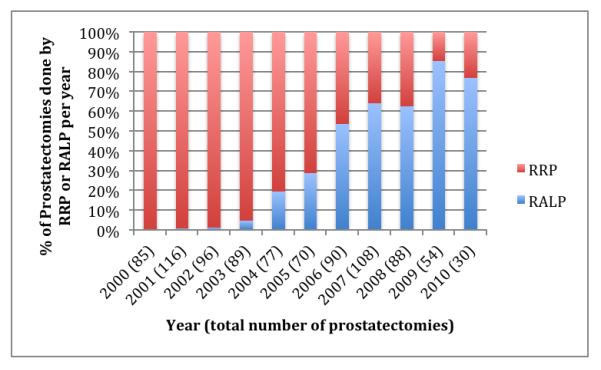
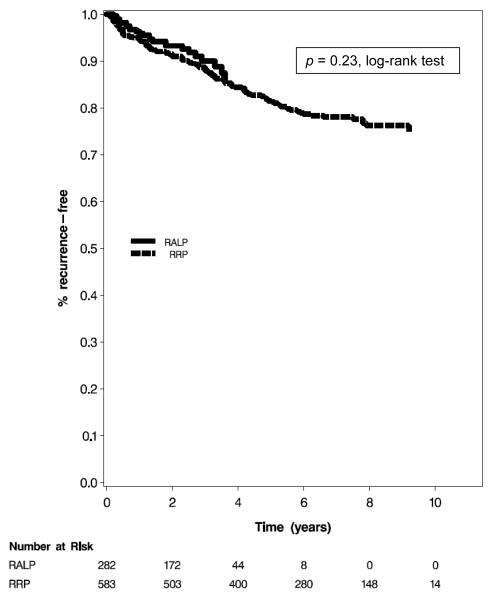
Results and limitations: Use of RALP increased during the study period, constituting 85.2% of study subjects in 2009, up from 4.5% in 2003. Patients undergoing RALP compared to RRP were less likely to have a lymph node dissection (51.5% vs 85.4%; p<0.0001), had less blood loss (207.4 ml vs 852.3 ml; p<0.0001), were less likely to receive blood transfusions (4.3% vs 30.3%; p<0.0001), and had shorter hospital stays (1.8 d vs 2.9 d; p<0.0001). Surgical, oncologic, and HRQOL outcomes did not differ significantly among the groups. In multivariate logistic regression models, there were no significant differences in 3- or 5-yr recurrence-free survival comparing RALP versus RRP (hazard ratios: 0.98 [95% confidence interval (CI), 0.46-2.08] and 0.75 [95% CI, 0.18-3.11], respectively).
Conclusions: In a nationwide cohort of patients undergoing surgical treatment for prostate cancer, RALP was associated with shorter hospital stay, and lower blood loss and transfusion rates than RRP. Surgical oncologic and HRQOL outcomes were similar between groups.
Patient summary: We studied men throughout the United States with prostate cancer who underwent surgical removal of the prostate. We found that robot-assisted laparoscopic radical prostatectomy resulted in shorter hospital stay, less blood loss, and fewer blood transfusions than radical retropubic prostatectomy. There were no differences in cancer control or health-related quality of life.
Keywords: Health-related quality of life; Open; Outcomes; Prostatectomy; Robotic.
Copyright © 2014 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
The controversy that will not go away.Eur Urol. 2015 Mar;67(3):439-40. doi: 10.1016/j.eururo.2014.02.052. Epub 2014 Mar 4. Eur Urol. 2015. PMID: 24631405 No abstract available.
Similar articles
-
Comparison of Acute Kidney Injury After Robot-Assisted Laparoscopic Radical Prostatectomy Versus Retropubic Radical Prostatectomy: A Propensity Score Matching Analysis.Medicine (Baltimore). 2016 Feb;95(5):e2650. doi: 10.1097/MD.0000000000002650. Medicine (Baltimore). 2016. PMID: 26844486 Free PMC article.
-
Functional and Oncological Outcomes After Open Versus Robot-assisted Laparoscopic Radical Prostatectomy for Localised Prostate Cancer: 8-Year Follow-up.Eur Urol. 2021 Nov;80(5):650-660. doi: 10.1016/j.eururo.2021.07.025. Epub 2021 Sep 15. Eur Urol. 2021. PMID: 34538508
-
Urinary Incontinence and Erectile Dysfunction After Robotic Versus Open Radical Prostatectomy: A Prospective, Controlled, Nonrandomised Trial.Eur Urol. 2015 Aug;68(2):216-25. doi: 10.1016/j.eururo.2015.02.029. Epub 2015 Mar 12. Eur Urol. 2015. PMID: 25770484 Clinical Trial.
-
Retzius-sparing versus standard robotic-assisted laparoscopic prostatectomy for the treatment of clinically localized prostate cancer.Cochrane Database Syst Rev. 2020 Aug 18;8(8):CD013641. doi: 10.1002/14651858.CD013641.pub2. Cochrane Database Syst Rev. 2020. PMID: 32813279 Free PMC article.
-
Retropubic, laparoscopic, and robot-assisted radical prostatectomy: a systematic review and cumulative analysis of comparative studies.Eur Urol. 2009 May;55(5):1037-63. doi: 10.1016/j.eururo.2009.01.036. Epub 2009 Jan 25. Eur Urol. 2009. PMID: 19185977
Cited by
-
Postprostatectomy Erectile Dysfunction: A Review.World J Mens Health. 2016 Aug;34(2):73-88. doi: 10.5534/wjmh.2016.34.2.73. Epub 2016 Aug 23. World J Mens Health. 2016. PMID: 27574591 Free PMC article. Review.
-
Cryopreserved placental tissue allograft accelerates time to continence following robot-assisted radical prostatectomy.J Robot Surg. 2021 Dec;15(6):877-883. doi: 10.1007/s11701-020-01187-z. Epub 2021 Jan 11. J Robot Surg. 2021. PMID: 33426577
-
Facility-level analysis of robot utilization across disciplines in the National Cancer Database.J Robot Surg. 2019 Apr;13(2):293-299. doi: 10.1007/s11701-018-0855-9. Epub 2018 Jul 30. J Robot Surg. 2019. PMID: 30062641
-
Biochemical recurrence after radical prostatectomy: Current status of its use as a treatment endpoint and early management strategies.Indian J Urol. 2019 Jan-Mar;35(1):6-17. doi: 10.4103/iju.IJU_355_18. Indian J Urol. 2019. PMID: 30692719 Free PMC article. Review.
-
Comparison of robotic and open radical prostatectomy: Initial experience of a single surgeon.Pak J Med Sci. 2021 Jan-Feb;37(1):167-174. doi: 10.12669/pjms.37.1.2719. Pak J Med Sci. 2021. PMID: 33437271 Free PMC article.
References
-
- Duffey B, Varda B, Konety B. Quality of evidence to compare outcomes of open and robot-assisted laparoscopic prostatectomy. Curr Urol Rep. 2011;12:229–36. - PubMed
-
- Kang DC, Hardee MJ, Fesperman SF, Stoffs TL, Dahm P. Low quality of evidence for robot-assisted laparoscopic prostatectomy: results of a systematic review of the published literature. Eur Urol. 2010;57:930–7. - PubMed
-
- Ficarra V, Novara G, Artibani W, et al. Retropubic, laparoscopic, and robot-assisted radical prostatectomy: a systematic review and cumulative analysis of comparative studies. Eur Urol. 2009;55:1037–63. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
