

A randomized trial of deferred stenting versus immediate stenting to prevent no- or slow-reflow in acute ST-segment elevation myocardial infarction (DEFER-STEMI)
- PMID: 24583294
- PMCID: PMC4029071
- DOI: 10.1016/j.jacc.2014.02.530
A randomized trial of deferred stenting versus immediate stenting to prevent no- or slow-reflow in acute ST-segment elevation myocardial infarction (DEFER-STEMI)
Abstract
Objectives: The aim of this study was to assess whether deferred stenting might reduce no-reflow and salvage myocardium in primary percutaneous coronary intervention (PCI) for ST-segment elevation myocardial infarction (STEMI).
Background: No-reflow is associated with adverse outcomes in STEMI.
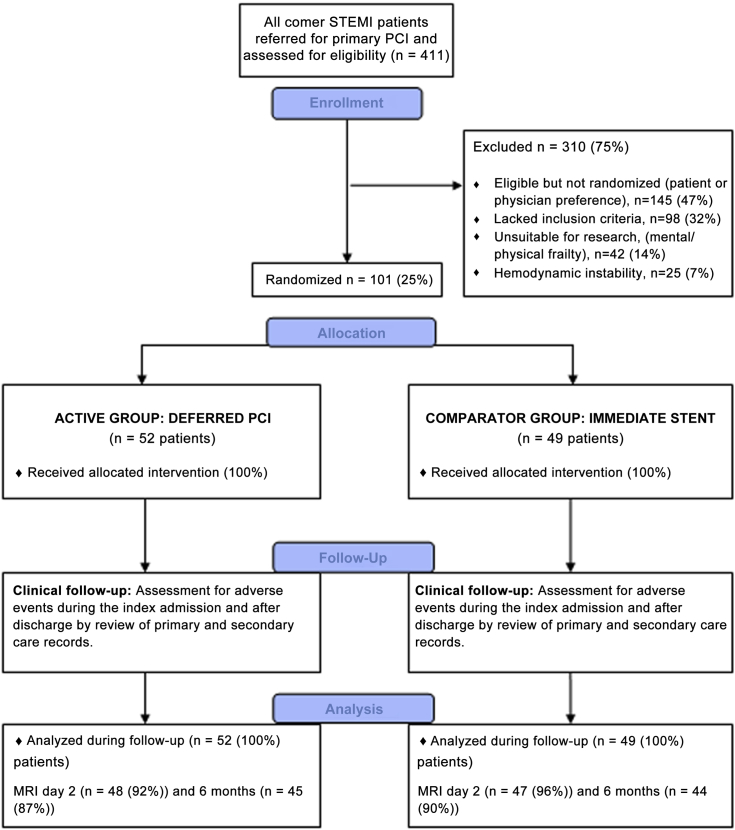
Methods: This was a prospective, single-center, randomized, controlled, proof-of-concept trial in reperfused STEMI patients with ≥1 risk factors for no-reflow. Randomization was to deferred stenting with an intention-to-stent 4 to 16 h later or conventional treatment with immediate stenting. The primary outcome was the incidence of no-/slow-reflow (Thrombolysis In Myocardial Infarction ≤2). Cardiac magnetic resonance imaging was performed 2 days and 6 months after myocardial infarction. Myocardial salvage was the final infarct size indexed to the initial area at risk.
Results: Of 411 STEMI patients (March 11, 2012 to November 21, 2012), 101 patients (mean age, 60 years; 69% male) were randomized (52 to the deferred stenting group, 49 to the immediate stenting). The median (interquartile range [IQR]) time to the second procedure in the deferred stenting group was 9 h (IQR: 6 to 12 h). Fewer patients in the deferred stenting group had no-/slow-reflow (14 [29%] vs. 3 [6%]; p = 0.006), no reflow (7 [14%] vs. 1 [2%]; p = 0.052) and intraprocedural thrombotic events (16 [33%] vs. 5 [10%]; p = 0.010). Thrombolysis In Myocardial Infarction coronary flow grades at the end of PCI were higher in the deferred stenting group (p = 0.018). Recurrent STEMI occurred in 2 patients in the deferred stenting group before the second procedure. Myocardial salvage index at 6 months was greater in the deferred stenting group (68 [IQR: 54% to 82%] vs. 56 [IQR: 31% to 72%]; p = 0.031].
Conclusions: In high-risk STEMI patients, deferred stenting in primary PCI reduced no-reflow and increased myocardial salvage. (Deferred Stent Trial in STEMI; NCT01717573).
Keywords: deferred stenting; myocardial infarction; myocardial salvage; no-reflow; primary percutaneous coronary intervention.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Put off till tomorrow what you can do today.J Am Coll Cardiol. 2014 May 27;63(20):2099-2100. doi: 10.1016/j.jacc.2014.01.056. Epub 2014 Mar 5. J Am Coll Cardiol. 2014. PMID: 24613320 No abstract available.
References
-
- Keeley E.C., Boura J.A., Grines C.L. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomized trials. Lancet. 2003;361:13–20. - PubMed
-
- O'Gara P.T., Kushner F.G., Ascheim D.D., et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61:485–510. - PubMed
-
- Jaffe R., Charron T., Puley G., Dick A., Strauss B.H. Microvascular obstruction and the no-reflow phenomenon after percutaneous coronary intervention. Circulation. 2008;117:3152–3156. - PubMed
-
- Morishima I., Sone T., Okumura K., et al. Angiographic no-reflow phenomenon as a predictor of adverse long-term outcome in patients treated with percutaneous transluminal coronary angioplasty for first acute myocardial infarction. J Am Coll Cardiol. 2000;36:1202–1209. - PubMed
-
- Antoniucci D., Valenti R., Migliorini A., et al. Direct infarct artery stenting without predilation and no-reflow in patients with acute myocardial infarction. Am Heart J. 2001;142:684–690. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
