

Bone loss from high repetitive high force loading is prevented by ibuprofen treatment
- PMID: 24583543
- PMCID: PMC4067254
Bone loss from high repetitive high force loading is prevented by ibuprofen treatment
Abstract
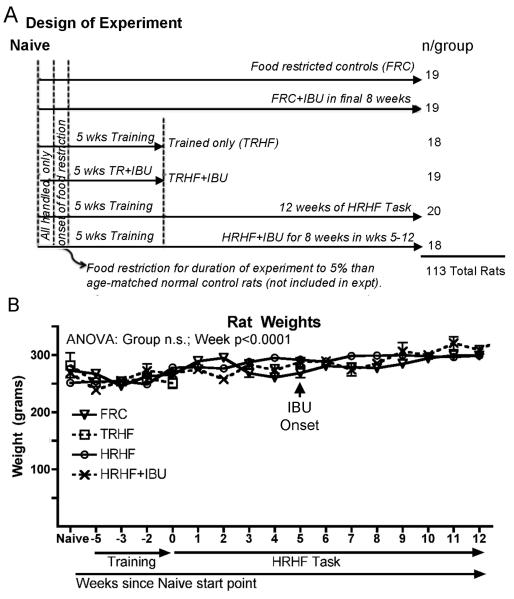
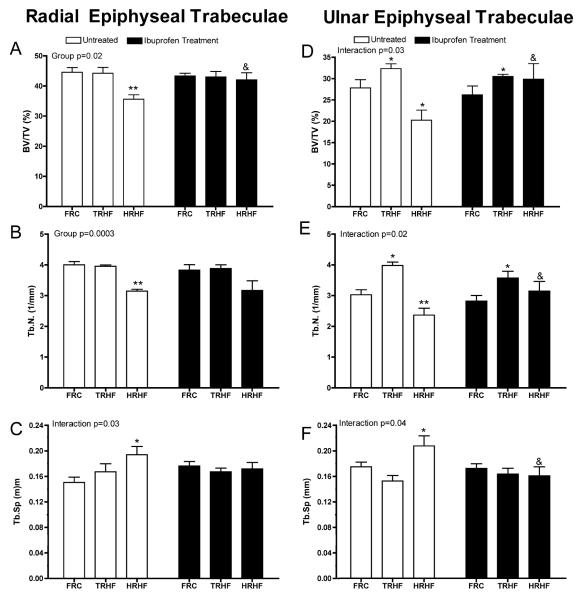
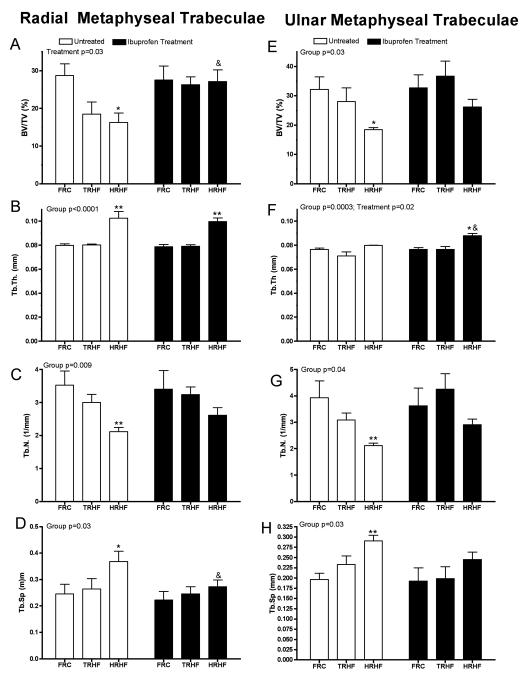
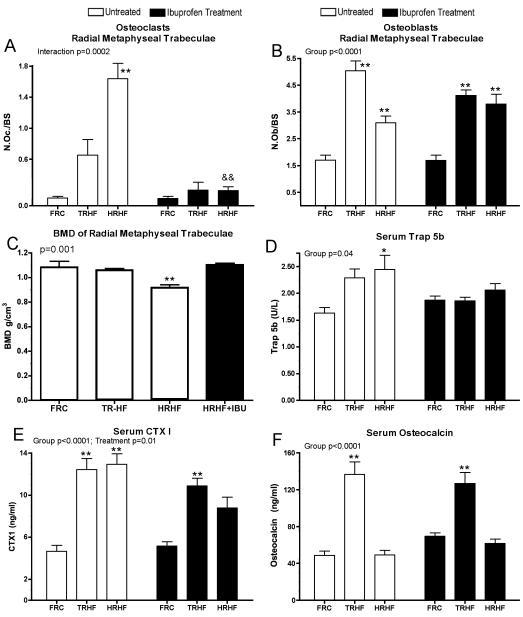
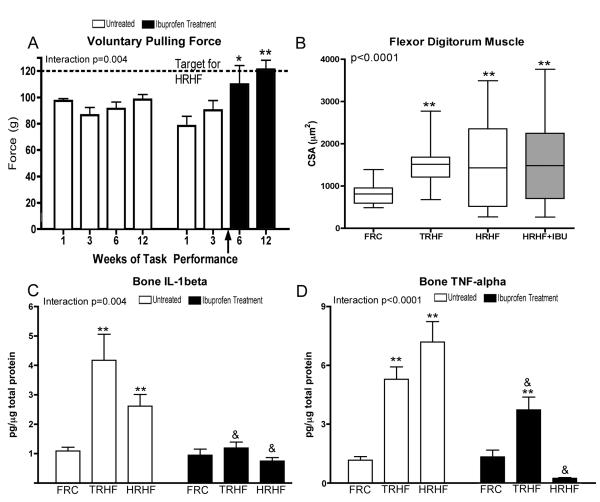
We examined roles of loading and inflammation on forearm bones in a rat model of upper extremity overuse. Trabecular structure in distal radius and ulna was examined in three groups of young adult rats: 1) 5% food-restricted that underwent an initial training period of 10 min/day for 5 weeks to learn the repetitive task (TRHF); 2) rats that underwent the same training before performing a high repetition high force task, 2 hours/day for 12 weeks (HRHF); and 3) food-restricted only (FRC). Subsets were treated with oral ibuprofen (IBU). TRHF rats had increased trabecular bone volume and numbers, osteoblasts, and serum osteocalcin, indicative of bone adaptation. HRHF rats had constant muscle pulling forces, showed limited signs of bone adaptation, but many signs of bone resorption, including decreased trabecular bone volume and bone mineral density, increased osteoclasts and bone inflammatory cytokines, and reduced median nerve conduction velocity (15%). HRHF+IBU rats showed no trabecular resorptive changes, no increased osteoclasts or bone inflammatory cytokines, no nerve inflammation, preserved nerve conduction, and increased muscle voluntary pulling forces. Ibuprofen treatment preserved trabecular bone quality by reducing osteoclasts and bone inflammatory cytokines, and improving muscle pulling forces on bones as a result of reduced nerve inflammation.
Figures


Similar articles
-
Effectiveness of conservative interventions for sickness and pain behaviors induced by a high repetition high force upper extremity task.BMC Neurosci. 2017 Mar 29;18(1):36. doi: 10.1186/s12868-017-0354-3. BMC Neurosci. 2017. PMID: 28356066 Free PMC article.
-
Ergonomic task reduction prevents bone osteopenia in a rat model of upper extremity overuse.Ind Health. 2015;53(3):206-21. doi: 10.2486/indhealth.2014-0159. Epub 2015 Feb 9. Ind Health. 2015. PMID: 25739896 Free PMC article.
-
Blocking CCN2 preferentially inhibits osteoclastogenesis induced by repetitive high force bone loading.Connect Tissue Res. 2021 Jan;62(1):115-132. doi: 10.1080/03008207.2020.1788546. Epub 2020 Jul 20. Connect Tissue Res. 2021. PMID: 32683988 Free PMC article.
-
Prolonged performance of a high repetition low force task induces bone adaptation in young adult rats, but loss in mature rats.Exp Gerontol. 2015 Dec;72:204-17. doi: 10.1016/j.exger.2015.10.014. Epub 2015 Oct 27. Exp Gerontol. 2015. PMID: 26517953 Free PMC article.
-
The interaction of force and repetition on musculoskeletal and neural tissue responses and sensorimotor behavior in a rat model of work-related musculoskeletal disorders.BMC Musculoskelet Disord. 2013 Oct 25;14:303. doi: 10.1186/1471-2474-14-303. BMC Musculoskelet Disord. 2013. PMID: 24156755 Free PMC article.
Cited by
-
Manual therapy prevents onset of nociceptor activity, sensorimotor dysfunction, and neural fibrosis induced by a volitional repetitive task.Pain. 2019 Mar;160(3):632-644. doi: 10.1097/j.pain.0000000000001443. Pain. 2019. PMID: 30461558 Free PMC article.
-
Blocking substance P signaling reduces musculotendinous and dermal fibrosis and sensorimotor declines in a rat model of overuse injury.Connect Tissue Res. 2020 Nov;61(6):604-619. doi: 10.1080/03008207.2019.1653289. Epub 2019 Aug 23. Connect Tissue Res. 2020. PMID: 31443618 Free PMC article.
-
Manual Therapy With Rest as a Treatment for Established Inflammation and Fibrosis in a Rat Model of Repetitive Strain Injury.Front Physiol. 2021 Nov 4;12:755923. doi: 10.3389/fphys.2021.755923. eCollection 2021. Front Physiol. 2021. PMID: 34803739 Free PMC article.
-
Occupational Activities: Factors That Tip the Balance From Bone Accrual to Bone Loss.Exerc Sport Sci Rev. 2020 Apr;48(2):59-66. doi: 10.1249/JES.0000000000000217. Exerc Sport Sci Rev. 2020. PMID: 32004169 Free PMC article. Review.
-
Risk factors and the natural history of accelerated knee osteoarthritis: a narrative review.BMC Musculoskelet Disord. 2020 May 29;21(1):332. doi: 10.1186/s12891-020-03367-2. BMC Musculoskelet Disord. 2020. PMID: 32471412 Free PMC article. Review.
References
-
- Bureau of Labor Statistics [November 8, 2012];Nonfatal ocupational injuries and illnesses requiring days away from work. News Release USDL-12-2204. 2011 http://www.bls.gov/news.release/osh2.nr0.htm. 2012.
-
- Werner RA, Franzblau A, Gell N, Ulin SS, Armstrong TJ. Predictors of upper extremity discomfort: a longitudinal study of industrial and clerical workers. Journal of occupational rehabilitation. 2005 Mar;15(1):27–35. - PubMed
-
- Bernard B. Musculoskeletal disorders and workplace factors. NIOSH Report 97–141, National Institute for Occupational Safety and Health; Cincinatti, Ohio, USA: 1997.
-
- Srilatha MAG, Bhat V, Sathiakumar N. Prevalence of Work-Related Wrist and Hand Musculoskeletal Disorders (WMSD) among Computer Users, Karnataka State, India. Journal of Clinical and Diagnostic Research. 2011 Jun;5(3):605–607.
-
- Ratzlaff CR, Gillies JH, Koehoorn MW. Work-related repetitive strain injury and leisure-time physical activity. Arthritis and rheumatism. 2007 Apr 15;57(3):495–500. - PubMed