

Genotypic resistance profiles of HIV-2-treated patients in West Africa
- PMID: 24583671
- PMCID: PMC4112041
- DOI: 10.1097/QAD.0000000000000244
Genotypic resistance profiles of HIV-2-treated patients in West Africa
Abstract
Objective: To assess the virological response, genotypic resistance profiles, and antiretroviral plasma concentrations in HIV-2 antiretroviral-treated (antiretroviral therapy, ART) patients in Côte d'Ivoire.
Methods: A cross-sectional survey was conducted among HIV-2 patients receiving ART. Plasma HIV-2 viral load was performed using the Agence Nationale de Recherche sur le SIDA et les hépatites virales (ANRS) assay. Protease and reverse transcriptase sequencing was performed using in-house methods and antiretroviral plasma concentrations were assessed using ultra performance liquid chromatography combined with tandem mass spectrometry.
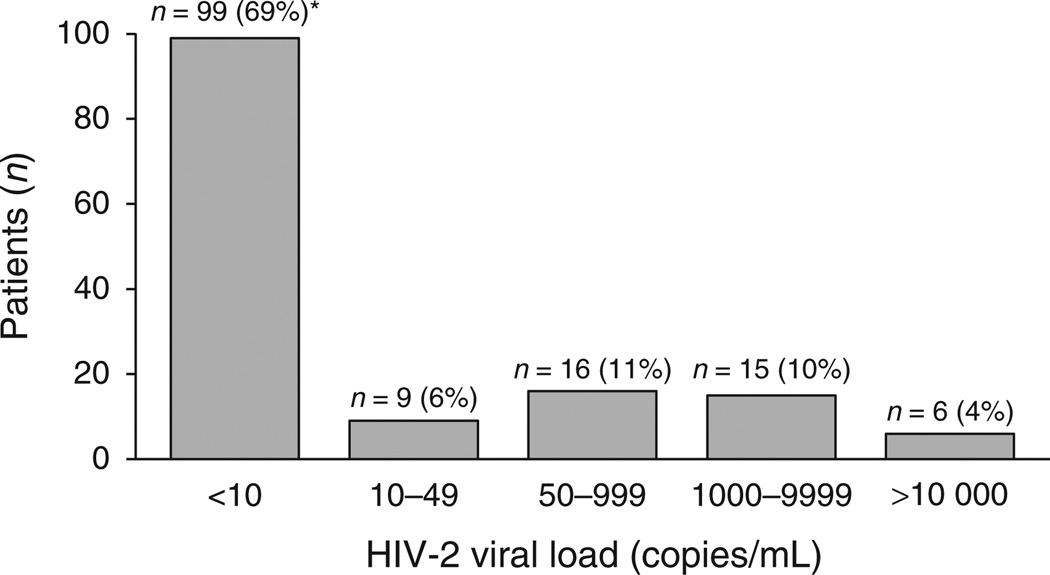
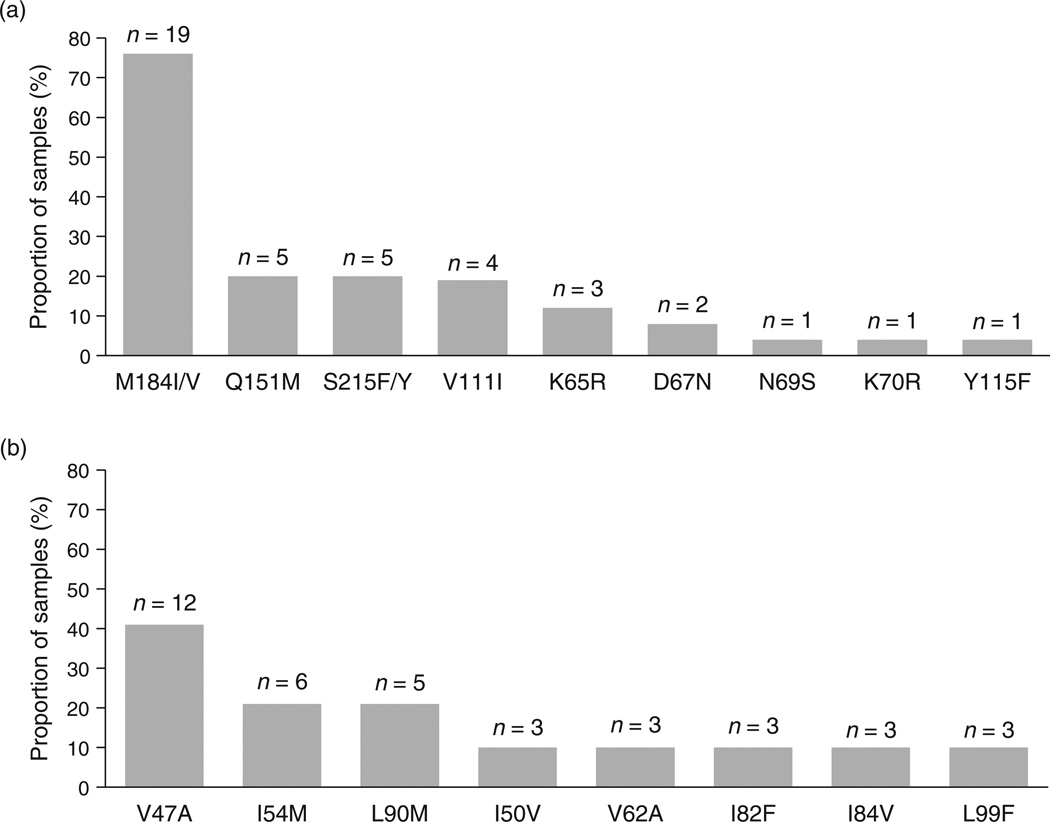
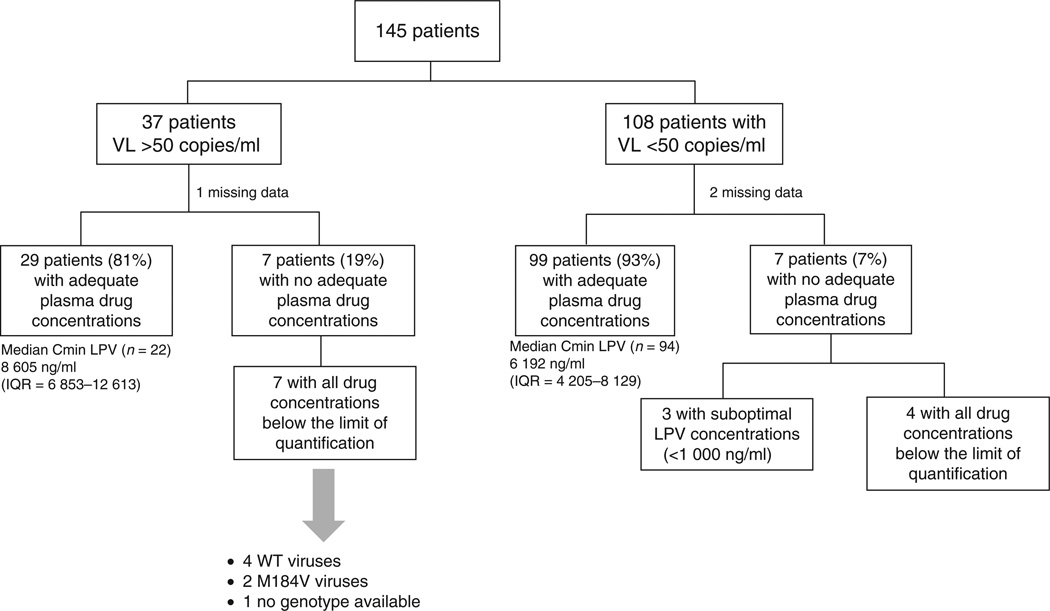
Results: One hundred and forty-five HIV-2-treated patients were enrolled with a median CD4 cell count of 360 cells/μl (interquartile range, IQR = 215-528). Median duration of ART was 4 years (IQR = 2-7) and 74% of patients displayed viral load less than 50 copies/ml. Median plasma HIV-2 RNA among patients with viral load more than 50 copies/ml was 3016 copies/ml (IQR = 436-5156). Most patients (84%) received a lopinavir/ritonavir-based regimen. HIV-2 resistance mutations to nucleoside reverse transcriptase inhibitors and protease inhibitors were detected in 21 of 25 (84%) and 20 of 29 (69%) samples, respectively. The most prevalent nucleoside reverse transcriptase inhibitor resistance mutations were M184I/V (90%), Q151M (24%), and S215F/Y (24%). The most prevalent protease inhibitor resistance mutations were V47A (60%) and I54M (30%). Median CD4 cell counts were 434 cells/μl (292-573) and 204 cells/μl (122-281) in patients with viral load less than 50 copies/ml and those exhibiting virological failure (P < 0.0001), respectively. The proportions of patients with adequate antiretroviral plasma concentrations were 81 and 93% in patients displaying virological failure and in those with viral load less than 50 copies/ml, respectively (P = 0.046), suggesting good treatment adherence.
Conclusion: We observed adequate drug plasma concentrations and virological suppression in a high proportion of HIV-2-infected patients. However, in cases of virological failure, the limited HIV-2 therapeutic arsenal and cross-resistance dramatically reduced treatment options.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- UNAIDS AIDS epidemic update 2006. Geneva, Switzerland: Joint United Nations Programme on HIV/AIDS (UNAIDS) and World Health Organization (WHO); 2004; 2006. pp. 1–94.
-
- Marlink R, Kanki P, Thior I, Travers K, Eisen G, Siby T, et al. Reduced rate of disease development after HIV-2 infection as compared to HIV-1. Science. 1994;265:1587–1590. - PubMed
-
- Popper SJ, Sarr AD, Travers KU, Guèye-Ndiaye A, Mboup S, Essex ME, et al. Lower human immunodeficiency virus (HIV) type 2 viral load reflects the difference in pathogenicity of HIV-1 and HIV-2. J Infect Dis. 1999;180 1116-01121. - PubMed
-
- Kanki PJ, Travers KU, MBoup S, Hsieh CC, Marlink RG, Gueye-NDiaye A, et al. Slower heterosexual spread of HIV-2 than HIV-1. Lancet. 1994;343:943–946. - PubMed
-
- Burgard M, Jasseron C, Matheron S, Damond F, Hamrene K, Blanche S, et al. Mother-to-child transmission of HIV-2 infection from 1986 to 2007 in the ANRS French Perinatal Cohort EPF-CO1. Clin Infect Dis. 2010;51:833–843. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
