

Intrarectal negative pressure system in the management of open abdomen with colorectal fistula: A case report
- PMID: 24584042
- PMCID: PMC3955241
- DOI: 10.1016/j.ijscr.2014.01.006
Intrarectal negative pressure system in the management of open abdomen with colorectal fistula: A case report
Abstract
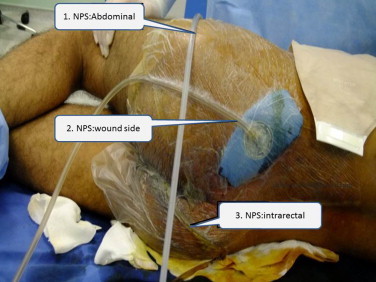
Introduction: To present the management of open abdomen with colorectal fistula by application of intrarectal negative pressure system (NPS) in addition to abdominal NPS.
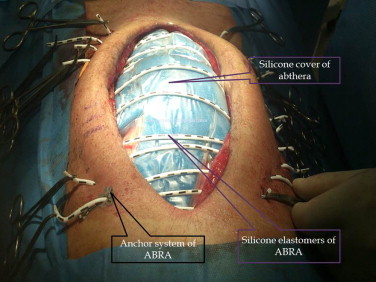
Presentation of case: Twenty-year old man had a history of injuries by a close-range gunshot to the abdomen eight days ago and he had been treated by bowel repairs, resections, jejunal anastomosis and Hartman's procedure. He was referred to our center after deterioration, evisceration with open abdomen and enteric fistula in septic shock. There were edematous, fibrinous bowels and large multiple fistulas from the edematous rectal stump. APACHE II, Mannheim Peritoneal Index and Björck scores were 18, 33 and 3, respectively (expected mortality 100%). After intensive care for 5 days, he was treated by abdominal and intrarectal NPS. NPS repeated for 5 times and the fistula was recovered on day 18 completely. Fascial closure was facilitated with a dynamic abdominal closure system (ABRA) and he was discharged on day 33 uneventfully. There was no herniation and any other problem after 12 months follow-up.
Discussion: Management of fistula in OA can be extremely challenging. Floating stoma, fistula VAC, nipple VAC, ring and silo VAC, fistula intubation systems are used for isolation of the enteric effluent from OA. Several biologic dressings such as acellular dermal matrix, pedicled flaps have been used to seal the fistula opening with various success. Resection of the involved enteric loop and a new anastomosis of the intestine is very hard and rarely possible. In all of these reports, usually patients are left to heal with a giant hernia. In contrast to this, there is no hernia in our case during one year follow up period.
Conclusion: Combination of intra and extra luminal negative pressure systems and ABRA is a safe and successful method to manage open abdomen with colorectal fistula.
Keywords: Colorectal fistula; Dynamic closure; Negative pressure; Open abdomen.
Copyright © 2014 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures







Similar articles
-
Management of fistula of ileal conduit in open abdomen by intra-condoit negative pressure system.Int J Surg Case Rep. 2014;5(7):385-8. doi: 10.1016/j.ijscr.2014.04.030. Epub 2014 May 9. Int J Surg Case Rep. 2014. PMID: 24858984 Free PMC article.
-
Delayed primary fascia closure of Björck grade 4 open abdomen with enteroatmospheric fistulas after repeated surgery for adhesive small bowel obstruction: a case report.BMC Surg. 2021 Aug 26;21(1):333. doi: 10.1186/s12893-021-01329-6. BMC Surg. 2021. PMID: 34452624 Free PMC article.
-
Combined management of open abdomen with enteroatmospheric fistula by negative pressure instill wound therapy and dermal matrix wound dressing.Ann Ital Chir. 2021 Jun 21;10:S2239253X21036367. Ann Ital Chir. 2021. PMID: 34193650
-
International consensus conference on open abdomen in trauma.J Trauma Acute Care Surg. 2016 Jan;80(1):173-83. doi: 10.1097/TA.0000000000000882. J Trauma Acute Care Surg. 2016. PMID: 27551925 Review.
-
"Enteroatmospheric fistulae"--gastrointestinal openings in the open abdomen: a review and recent proposal of a surgical technique.Scand J Surg. 2013;102(2):61-8. doi: 10.1177/1457496913482252. Scand J Surg. 2013. PMID: 23820678 Review.
Cited by
-
Two surgeons' collaboration to close an extreme open abdomen with loss of domain utilizing the abdominal dynamic tissue system and porcine urinary bladder matrix.Proc (Bayl Univ Med Cent). 2022 Jul 11;35(6):876-878. doi: 10.1080/08998280.2022.2092709. eCollection 2022. Proc (Bayl Univ Med Cent). 2022. PMID: 36304601 Free PMC article.
-
Management of Necrotizing Fasciitis and Fecal Peritonitis following Ostomy Necrosis and Detachment by Using NPT and Flexi-Seal.Case Rep Surg. 2015;2015:231450. doi: 10.1155/2015/231450. Epub 2015 Sep 10. Case Rep Surg. 2015. PMID: 26448894 Free PMC article.
-
Successful Treatment of a Large Pelvic Abscess Using Intraluminal VAC: A Case Report.J Clin Diagn Res. 2016 Apr;10(4):PD19-20. doi: 10.7860/JCDR/2016/18485.7659. Epub 2016 Apr 1. J Clin Diagn Res. 2016. PMID: 27190889 Free PMC article.
-
Management of a Septic Open Abdomen Patient with Spontaneous Jejunal Perforation after Emergent C/S with Confounding Factor of Mild Acute Pancreatitis.Case Rep Surg. 2016;2016:7153579. doi: 10.1155/2016/7153579. Epub 2016 Feb 23. Case Rep Surg. 2016. PMID: 27006853 Free PMC article.
-
Intra-abdominal Pressure Monitoring in Open Abdomen Management with Dynamic Abdominal Closure.Indian J Surg. 2017 Oct;79(5):384-389. doi: 10.1007/s12262-016-1491-0. Epub 2016 May 13. Indian J Surg. 2017. PMID: 29089695 Free PMC article.
References
-
- D’Hondt M., Devriendt D., Van Rooy F., Vansteenkiste F., D’Hoore A., Penninckx F. Treatment of small-bowel fistulae in the open abdomen with topical negative-pressure therapy. Am J Surg. 2011;202:20–24. - PubMed
-
- Marinis A., Gkiokas G., Argyra E., Fragulidis G., Polymeneas G., Voros D. “Enteroatmospheric fistulae”—gastrointestinal openings in the open abdomen: a review and recent proposal of a surgical technique. Scand J Surg. 2013;102(2):61–68. - PubMed
-
- Levy E., Frileux P., Cugnenc P.H., Parc R., Ollivier J.M., Honiger J. Exposed fistula of the small intestine, a complication of peritonitis or laparotomy. Apropos of 120 cases. Ann Chir. 1986;40:184–195. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
