

Removal of Different Classes of Uremic Toxins in APD vs CAPD: A Randomized Cross-Over Study
- PMID: 24584609
- PMCID: PMC4520726
- DOI: 10.3747/pdi.2013.00202
Removal of Different Classes of Uremic Toxins in APD vs CAPD: A Randomized Cross-Over Study
Abstract
♦
Aim: In this study, we investigated, and this for the different classes of uremic toxins, whether increasing dialysate volume by shifting from continuous ambulatory peritoneal dialysis (CAPD) to higher volume automated peritoneal dialysis (APD) increases total solute clearance. ♦
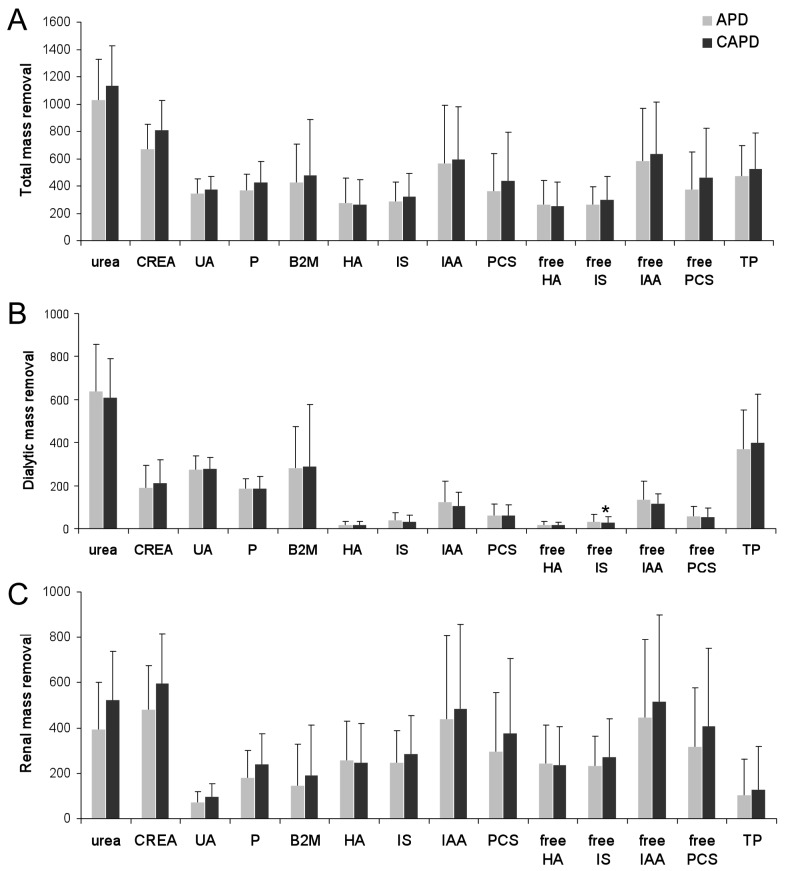
Methods: Patients on peritoneal dialysis were randomized in a cross-over design to one 24-hour session of first a CAPD regimen (3*2 L of Physioneal 1.36% and 1*2 L of icodextrin) or APD (consisting of 5 cycles of 2 L Physioneal 1.36 and 1 cycle of 2 L Extraneal), and the other week the alternate regime, each patient serving as his/her own control. Dialysate, blood and urine samples were collected and frozen for later batch analysis of concentrations of urea, creatinine, phosphorus, uric acid, hippuric acid, 3-carboxy-4-methyl-5-propyl-2-furanpropionic acid, indoxyl sulfate, indole acetic acid, and p-cresyl sulfate. For the protein-bound solutes, total and free fractions were determined. Total, peritoneal and renal clearance (K) and mass removal (MR) of each solute were calculated, using validated models. ♦
Results: In 15 patients (11 male, 3 diabetics, 56 ± 16 years, 8 on CAPD, time on peritoneal dialysis 12 ± 14 months, and residual renal function of 9.9 ± 5.4 mL/min) dialysate over plasma ratio for creatinine (D/Pcrea) was 0.62 ± 0.10. Drained volume and obtained ultrafiltration were higher with APD vs CAPD (13.3 ± 0.5 L vs 8.5 ± 0.7 L and 1.3 ± 0.5 L vs 0.5 ± 0.7 L), whereas urine output was lower (1.0 ± 0.5 L vs 1.4 ± 0.6 L). Total clearance and MR tended to be higher for CAPD vs APD for all small and water soluble solutes, but mainly because of higher renal contribution, with no difference in the peritoneal contribution. For the protein-bound solutes, no differences in clearance or mass removal were observed. ♦
Conclusion: Although the drained dialysate volume nearly doubled, APD did not result in better peritoneal clearance or solute removal vs classic CAPD. APD resulted in better ultrafiltration, but at the expense of residual urinary output and clearance.
Keywords: APD; CAPD; Uremic toxin; clearance; dwells; removal.
Copyright © 2015 International Society for Peritoneal Dialysis.
Figures
References
-
- Mehrotra R, Chiu YW, Kalantar-Zadeh K, Vonesh E. The outcomes of continuous ambulatory and automated peritoneal dialysis are similar. Kidney Int 2009; 76(1):97–107. - PubMed
-
- Badve SV, Hawley CM, McDonald SP, Mudge DW, Rosman JB, Brown FG, et al. Automated and continuous ambulatory peritoneal dialysis have similar outcomes. Kidney Int 2008; 73(4):480–8. - PubMed
-
- Johnson DW, Hawley CM, McDonald SP, Brown FG, Rosman JB, Wiggins KJ, et al. Superior survival of high transporters treated with automated versus continuous ambulatory peritoneal dialysis. Nephrol Dial Transplant 2010; 25(6):1973–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
