

Incident HIV during pregnancy and postpartum and risk of mother-to-child HIV transmission: a systematic review and meta-analysis
- PMID: 24586123
- PMCID: PMC3934828
- DOI: 10.1371/journal.pmed.1001608
Incident HIV during pregnancy and postpartum and risk of mother-to-child HIV transmission: a systematic review and meta-analysis
Abstract
Background: Women may have persistent risk of HIV acquisition during pregnancy and postpartum. Estimating risk of HIV during these periods is important to inform optimal prevention approaches. We performed a systematic review and meta-analysis to estimate maternal HIV incidence during pregnancy/postpartum and to compare mother-to-child HIV transmission (MTCT) risk among women with incident versus chronic infection.
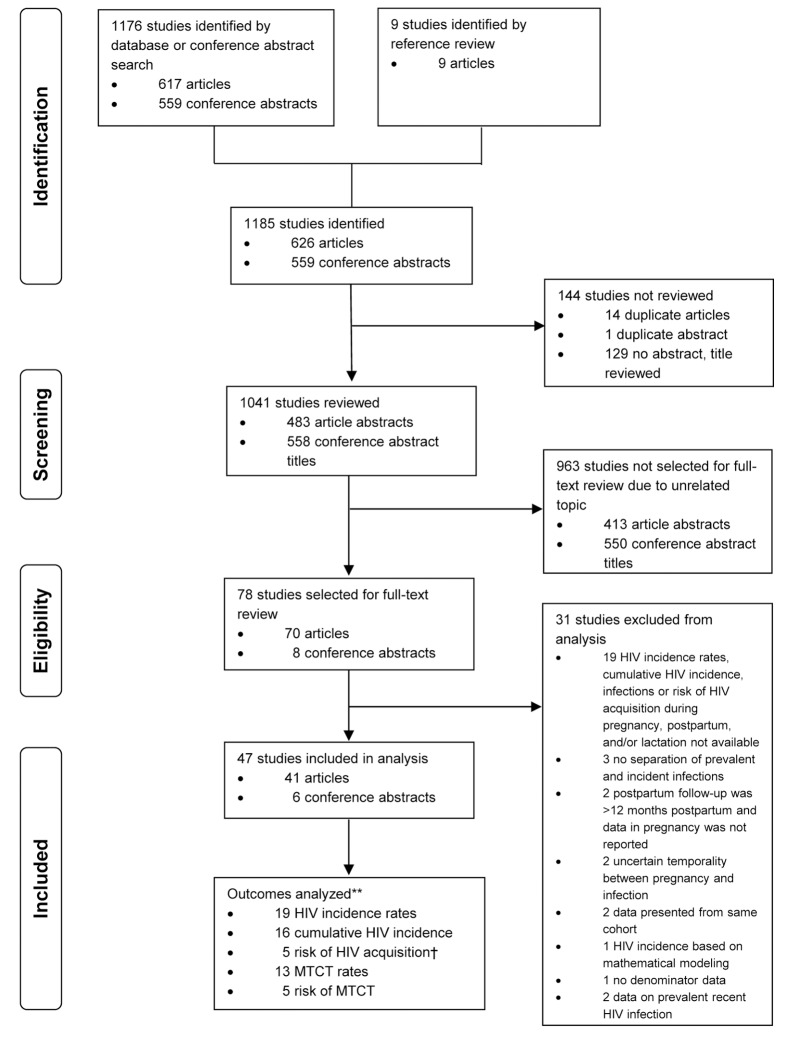
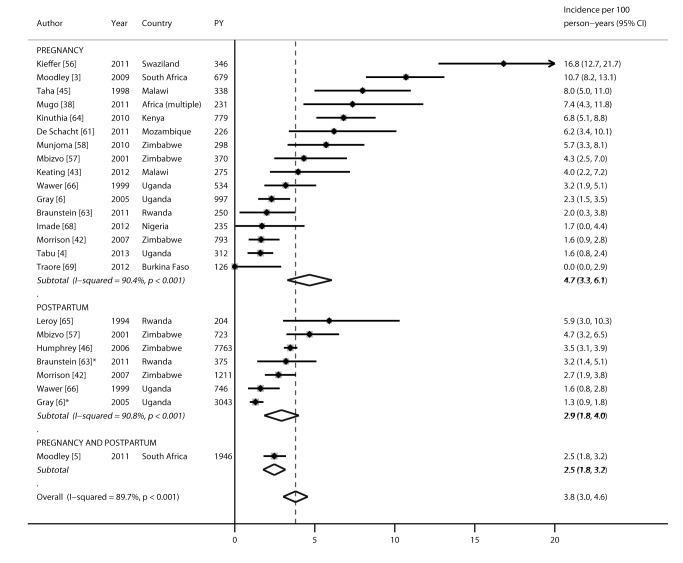
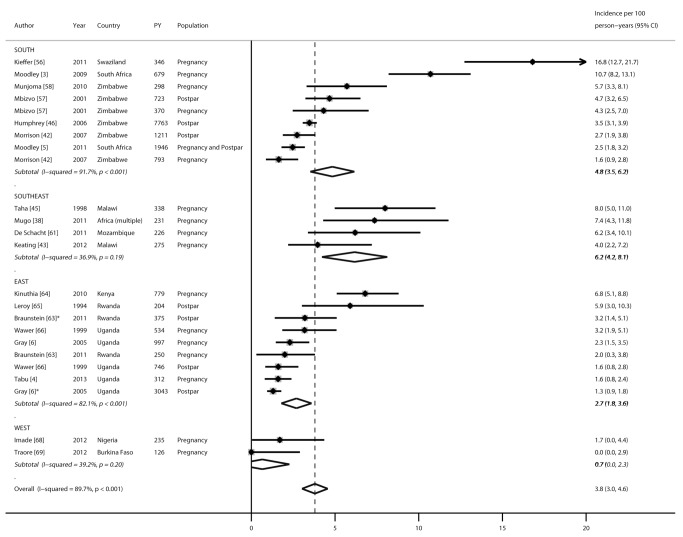
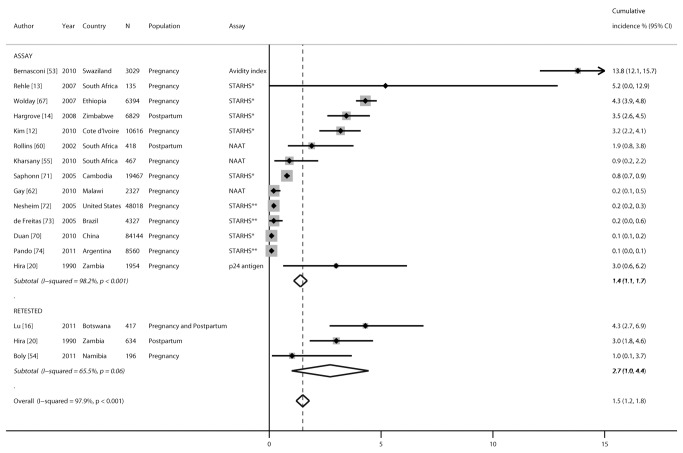
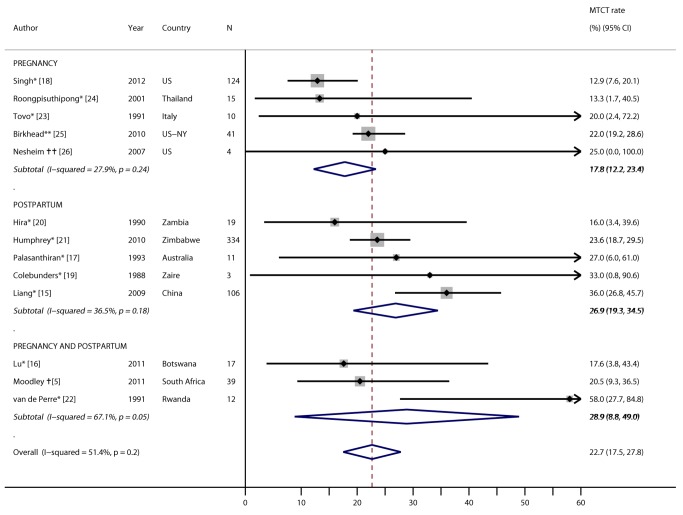
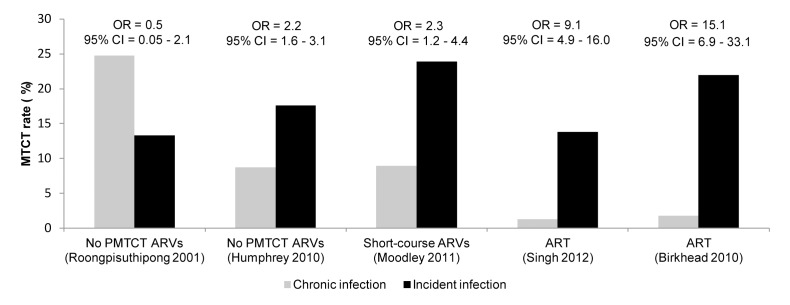
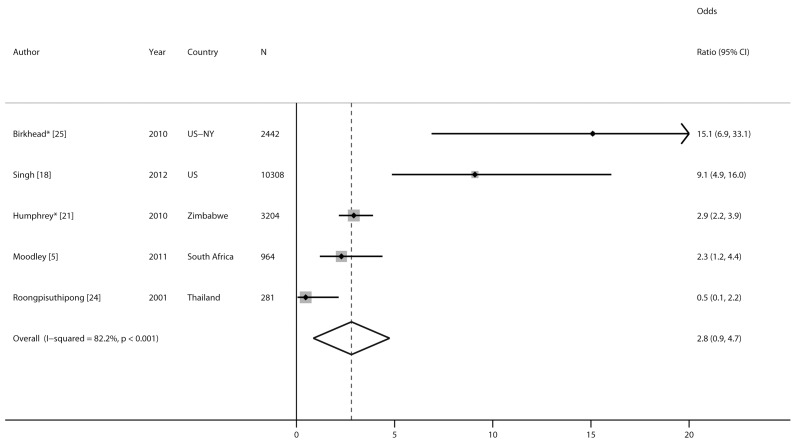
Methods and findings: We searched PubMed, Embase, and AIDS-related conference abstracts between January 1, 1980, and October 31, 2013, for articles and abstracts describing HIV acquisition during pregnancy/postpartum. The inclusion criterion was studies with data on recent HIV during pregnancy/postpartum. Random effects models were constructed to pool HIV incidence rates, cumulative HIV incidence, hazard ratios (HRs), or odds ratios (ORs) summarizing the association between pregnancy/postpartum status and HIV incidence, and MTCT risk and rates. Overall, 1,176 studies met the search criteria, of which 78 met the inclusion criterion, and 47 contributed data. Using data from 19 cohorts representing 22,803 total person-years, the pooled HIV incidence rate during pregnancy/postpartum was 3.8/100 person-years (95% CI 3.0-4.6): 4.7/100 person-years during pregnancy and 2.9/100 person-years postpartum (p = 0.18). Pooled cumulative HIV incidence was significantly higher in African than non-African countries (3.6% versus 0.3%, respectively; p<0.001). Risk of HIV was not significantly higher among pregnant (HR 1.3, 95% CI 0.5-2.1) or postpartum women (HR 1.1, 95% CI 0.6-1.6) than among non-pregnant/non-postpartum women in five studies with available data. In African cohorts, MTCT risk was significantly higher among women with incident versus chronic HIV infection in the postpartum period (OR 2.9, 95% CI 2.2-3.9) or in pregnancy/postpartum periods combined (OR 2.3, 95% CI 1.2-4.4). However, the small number of studies limited power to detect associations and sources of heterogeneity.
Conclusions: Pregnancy and the postpartum period are times of persistent HIV risk, at rates similar to "high risk" cohorts. MTCT risk was elevated among women with incident infections. Detection and prevention of incident HIV in pregnancy/postpartum should be prioritized, and is critical to decrease MTCT.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Perinatal HIV prevention aims for elimination. AIDS Read 12: 146, 150. - PubMed
-
- Branson BM, Handsfield HH, Lampe MA, Janssen RS, Taylor AW, et al. (2006) Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Recomm Rep 55: 1–17. - PubMed
-
- Moodley D, Esterhuizen TM, Pather T, Chetty V, Ngaleka L (2009) High HIV incidence during pregnancy: compelling reason for repeat HIV testing. AIDS 23: 1255–1259. - PubMed
-
- Tabu F, Ngonzi J, Mugyenyi G, Bajunirwe F, Mayanja R, et al. (2013) Prevalence of HIV infection among parturients with a negative primary test during the antenatal period at Mbarara Regional Referral Hospital, Uganda [abstract]. SpROGs 2013 Conference; 5–6 Dec 2013; Nottingham, United Kingdom.
-
- Moodley D, Esterhuizen T, Reddy L, Moodley P, Singh B, et al. (2011) Incident HIV infection in pregnant and lactating women and its effect on mother-to-child transmission in South Africa. J Infect Dis 203: 1231–1234. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
