

Transbronchial lung cryobiopsy in the diagnosis of fibrotic interstitial lung diseases
- PMID: 24586252
- PMCID: PMC3938401
- DOI: 10.1371/journal.pone.0086716
Transbronchial lung cryobiopsy in the diagnosis of fibrotic interstitial lung diseases
Abstract
Background: Histology is a key element for the multidisciplinary diagnosis of fibrotic diffuse parenchymal lung diseases (f-DPLD) when the clinical-radiological picture is nondiagnostic. Transbronchial lung cryobiopsy (TBLC) have been shown to be useful for obtaining large and well-preserved biopsies of lung parenchyma, but experience with TBLC in f-DPLD is limited.
Objectives: To evaluate safety, feasibility and diagnostic yield of TBLC in f-DPLD.
Method: Prospective study of 69 cases of TBLC using flexible cryoprobe in the clinical-radiological setting of f-DPLD with nondiagnostic high resolution computed tomography (HRCT) features.
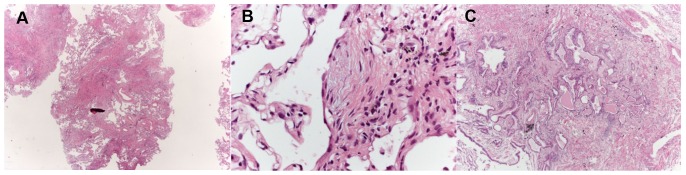
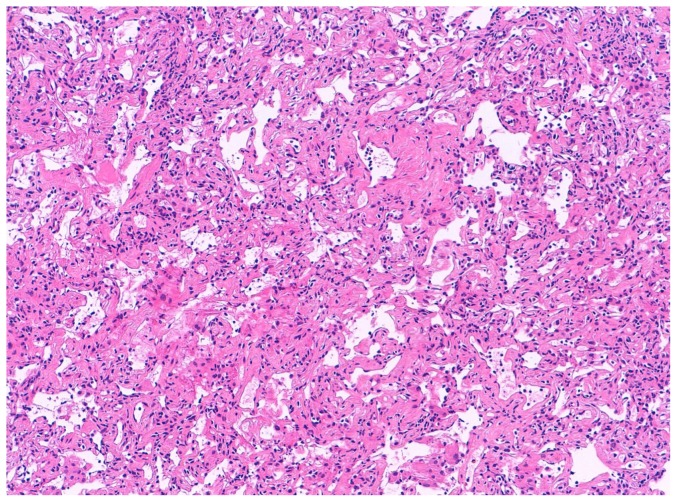
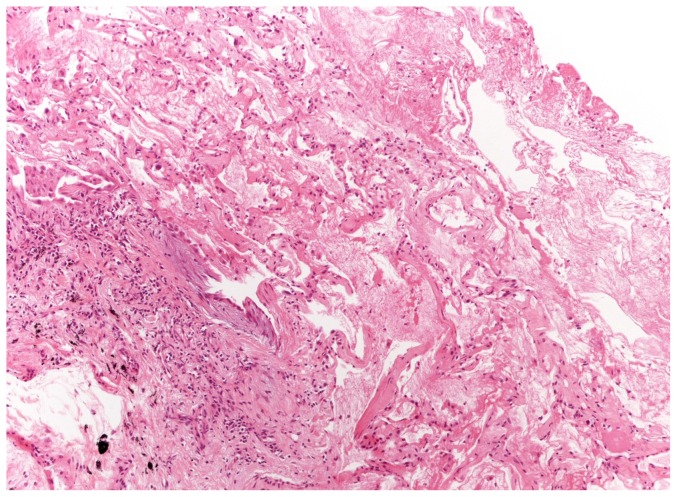
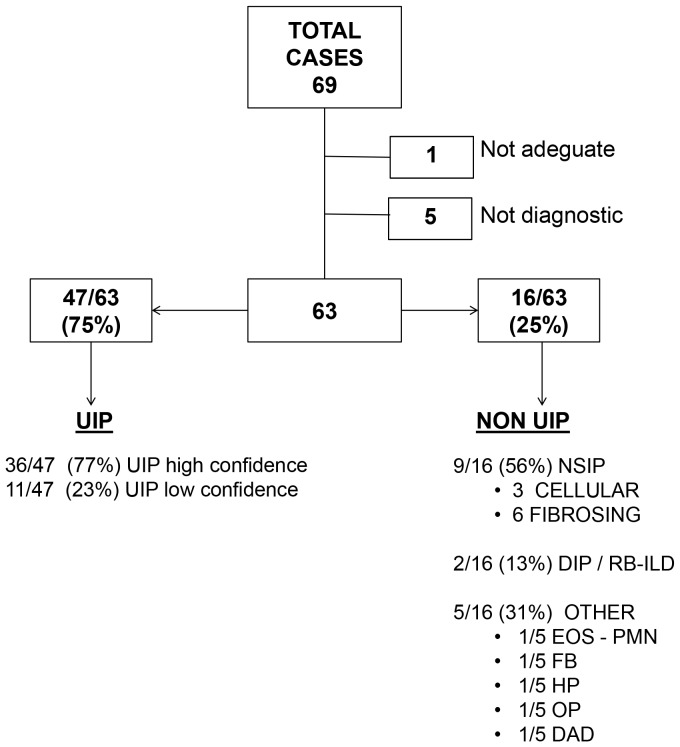
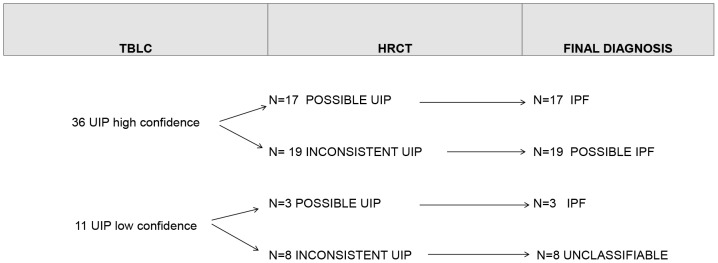
Safety: pneumothorax occurred in 19 patients (28%). One patient (1.4%) died of acute exacerbation. Feasibility: adequate cryobiopsies were obtained in 68 cases (99%). The median size of cryobiopsies was 43.11 mm(2) (range, 11.94-76.25). Diagnostic yield: among adequate TBLC the pathologists were confident ("high confidence") that histopathologic criteria sufficient to define a specific pattern in 52 patients (76%), including 36 of 47 with UIP (77%) and 9 nonspecific interstitial pneumonia (6 fibrosing and 3 cellular), 2 desquamative interstitial pneumonia/respiratory bronchiolitis-interstitial lung disease, 1 organizing pneumonia, 1 eosinophilic pneumonia, 1 diffuse alveolar damage, 1 hypersensitivity pneumonitis and 1 follicular bronchiolitis. In 11 diagnoses of UIP the pathologists were less confident ("low confidence"). Agreement between pathologists in the detection of UIP was very good with a Kappa coefficient of 0.83 (95% CI, 0.69-0.97). Using the current consensus guidelines for clinical-radiologic-pathologic correlation 32% (20/63) of cases were classified as Idiopathic Pulmonary Fibrosis (IPF), 30% (19/63) as possible IPF, 25% (16/63) as other f-DPLDs and 13% (8/63) were unclassifiable.
Conclusions: TBLC in the diagnosis of f-DPLD appears safe and feasible. TBLC has a good diagnostic yield in the clinical-radiological setting of f-DPLD without diagnostic HRCT features of usual interstitial pneumonia. Future studies should consider TBLC as a potential alternative to SLBx in f-DPLD.
Conflict of interest statement
Figures
References
-
- ATS/ERS Committee on Idiopathic Interstitial Pneumonias (2013) An official american thoracic society/european respiratory society statement: update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med 15;188: 733–48. - PMC - PubMed
-
- Sverzellati N, Wells AU, Tomassetti S, Desai SR, Copley SJ, et al. (2010) Biopsy-proved idiopathic pulmonary fibrosis: spectrum of nondiagnostic thin-section CT diagnoses. Radiology 254: 957–64. - PubMed
-
- Kreider ME, Hansen-Flaschen J, Ahmad NN, Rossman MD, Kaiser LR, et al. (2007) Complications of Video-Assisted Thoracoscopic Lung Biopsy in Patients with Interstitial Lung Disease. Ann Thorac Surg 83: 1140–5. - PubMed
-
- Kondoh Y, Taniguchi H, Kitaichi M, Yokoi T, Johkoh T, et al. (2006) Acute exacerbation of interstitial pneumonia following surgical lung biopsy. Respir Med 100: 1753–1759. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
