

The association between self-reported stigma and loss-to-follow up in treatment eligible HIV positive adults in rural Kwazulu-Natal, South Africa
- PMID: 24586310
- PMCID: PMC3930529
- DOI: 10.1371/journal.pone.0088235
The association between self-reported stigma and loss-to-follow up in treatment eligible HIV positive adults in rural Kwazulu-Natal, South Africa
Abstract
Background: The relationship between loss-to-follow-up (LTFU) in HIV treatment and care programmes and psychosocial factors, including self-reported stigma, is important to understand. This prospective cohort study explored stigma and LTFU in treatment eligible adults who had yet not started antiretroviral therapy (ART).
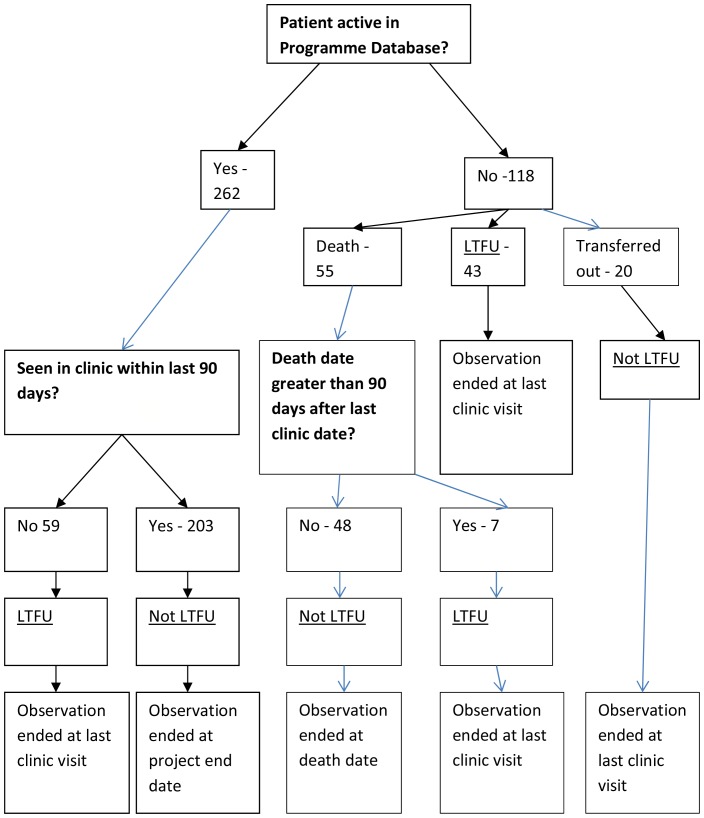
Methods: Psychosocial, clinical and demographic data were collected at a baseline interview. Self-reported stigma was measured with a multi-item scale. LTFU was defined as not attending clinic in the 90 days since last appointment or before death. Data was collected between January 2009 and January 2013 and analysed using Cox Regression.
Results: 380 individuals were recruited (median time in study 3.35 years, total time at risk 1065.81 person-years). 203 were retained (53.4%), 109 were LTFU (28.7%), 48 had died and were not LTFU at death (12.6%) and 20 had transferred out (5.3%). The LTFU rate was 10.65 per 100 person-years (95% CI: 8.48-12.34). 362 individuals (95.3%) started ART. Stigma total score (categorised in quartiles) was not significantly associated with LTFU in either univariable or multivariable analysis (adjusting for other variables in the final model): second quartile aHR 0.77 (95%CI: 0.41-1.46), third quartile aHR 1.20(95%CI: 0.721-2.04), fourth quartile aHR 0.62 (95%CI: 0.35-1.11). In the final multivariable model, higher LTFU rates were associated with male gender, increased openness with friends/family and believing that community problems would be solved at higher levels. Lower LTFU rates were independently associated with increased year of age, greater reliance on family/friends, and having children.
Conclusions: Demographic and other psychosocial factors were more closely related to LTFU than self-reported stigma. This may be consistent with high levels of social exposure to HIV and ART and with stigma affecting LTFU less than other stages of care. Research and clinical implications are discussed.
Conflict of interest statement
Similar articles
-
Factors associated with pre-ART loss-to-follow up in adults in rural KwaZulu-Natal, South Africa: a prospective cohort study.BMC Public Health. 2016 Apr 27;16:358. doi: 10.1186/s12889-016-3025-x. BMC Public Health. 2016. PMID: 27117271 Free PMC article.
-
Determinants of loss to follow-up among HIV positive patients receiving antiretroviral therapy in a test and treat setting: A retrospective cohort study in Masaka, Uganda.PLoS One. 2020 Apr 7;15(4):e0217606. doi: 10.1371/journal.pone.0217606. eCollection 2020. PLoS One. 2020. PMID: 32255796 Free PMC article.
-
Predictors of loss to follow-up among children in the first and second years of antiretroviral treatment in Johannesburg, South Africa.Glob Health Action. 2013 Jan 24;6:19248. doi: 10.3402/gha.v6i0.19248. Glob Health Action. 2013. PMID: 23364098 Free PMC article.
-
Same-day antiretroviral therapy is associated with increased loss to follow-up in South African public health facilities: a prospective cohort study of patients diagnosed with HIV.J Int AIDS Soc. 2020 Jun;23(6):e25529. doi: 10.1002/jia2.25529. J Int AIDS Soc. 2020. PMID: 32510186 Free PMC article.
-
Misreporting of Patient Outcomes in the South African National HIV Treatment Database: Consequences for Programme Planning, Monitoring, and Evaluation.Front Public Health. 2020 Apr 7;8:100. doi: 10.3389/fpubh.2020.00100. eCollection 2020. Front Public Health. 2020. PMID: 32318534 Free PMC article. Review.
Cited by
-
Towards an AIDS free generation: Is stigma still an issue in Zambia? Results from a legal environment assessment of the HIV/AIDS/TB program of the Churches Health Association of Zambia.J Public Health Afr. 2020 Mar 19;10(2):1010. doi: 10.4081/jphia.2019.1010. eCollection 2019 Dec 31. J Public Health Afr. 2020. PMID: 32257070 Free PMC article.
-
Exploring HIV-related stigma among HIV-infected men who have sex with men in Beijing, China: a correlation study.AIDS Care. 2016 Nov;28(11):1394-401. doi: 10.1080/09540121.2016.1179713. Epub 2016 May 3. AIDS Care. 2016. PMID: 27137205 Free PMC article.
-
Prevalence, trend and risk factors for antiretroviral therapy discontinuation among HIV-infected adults in Ethiopia in 2003-2015.PLoS One. 2017 Jun 16;12(6):e0179533. doi: 10.1371/journal.pone.0179533. eCollection 2017. PLoS One. 2017. PMID: 28622361 Free PMC article. Clinical Trial.
-
Exploring the Relationship Between Anticipated Stigma and Community Shared Concerns about HIV on Defaulting from HIV Care in Rural South Africa.Stigma Health. 2024 May;9(2):173-180. doi: 10.1037/sah0000475. Epub 2023 Aug 31. Stigma Health. 2024. PMID: 38983717 Free PMC article.
-
Predictors of loss to follow-up in antiretroviral treatment for adult patients in the Oromia region, Ethiopia.HIV AIDS (Auckl). 2016 Apr 26;8:83-92. doi: 10.2147/HIV.S98137. eCollection 2016. HIV AIDS (Auckl). 2016. PMID: 27175095 Free PMC article.
References
-
- UNAIDS (2009) South Africa: Country Situation.
-
- Shisana O (2013) HIV/AIDS in South Africa: At last the Glass is Half Full. South Africa Aids Conference. Durban, South Africa.
-
- Plazy M, Dray-Spira R, Orne-Gliemann J, Dabis F, Newell ML (2013) Retention in Care Up to ART initiation within a Decentralized HIV Programme in South Africa: the critical role of the 1st clinic visit. CROI. Atlanta, USA.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
