

Extended adjuvant tamoxifen for early breast cancer: a meta-analysis
- PMID: 24586311
- PMCID: PMC3930532
- DOI: 10.1371/journal.pone.0088238
Extended adjuvant tamoxifen for early breast cancer: a meta-analysis
Abstract
Background: Hormone receptor positive breast cancer is characterized by the potential for disease recurrence many years after initial diagnosis. Endocrine therapy has been shown to reduce the risk of such recurrence, but the optimal duration of endocrine therapy remains unclear.
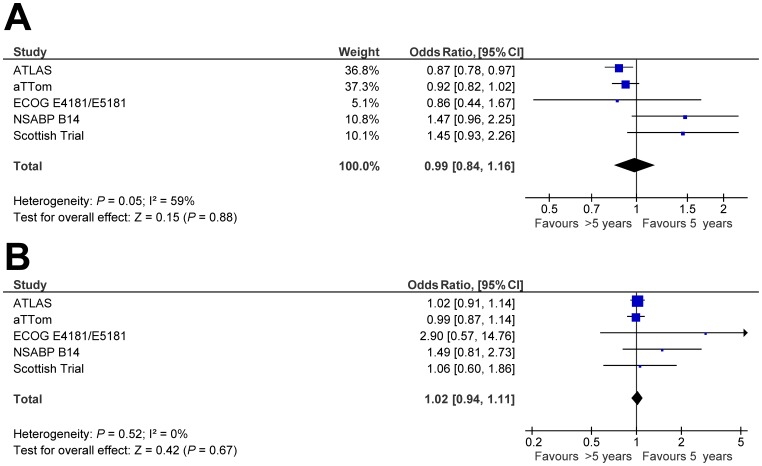
Methods: We conducted a systematic review and meta-analysis to quantify the benefits and harms of extended adjuvant tamoxifen (>5 years of therapy) compared with adjuvant tamoxifen (5 years of therapy). Odds ratios (ORs) and 95% confidence intervals (CIs) were computed for disease recurrence, death and adverse events. Subgroup analyses by timing of recurrence and baseline lymph node and menopause status were carried.
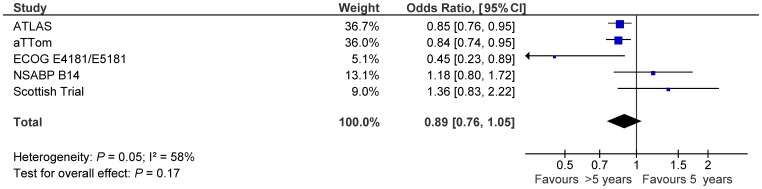
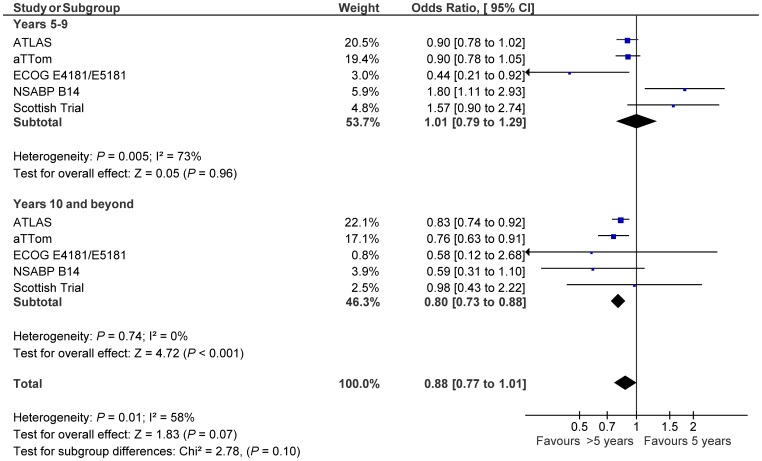
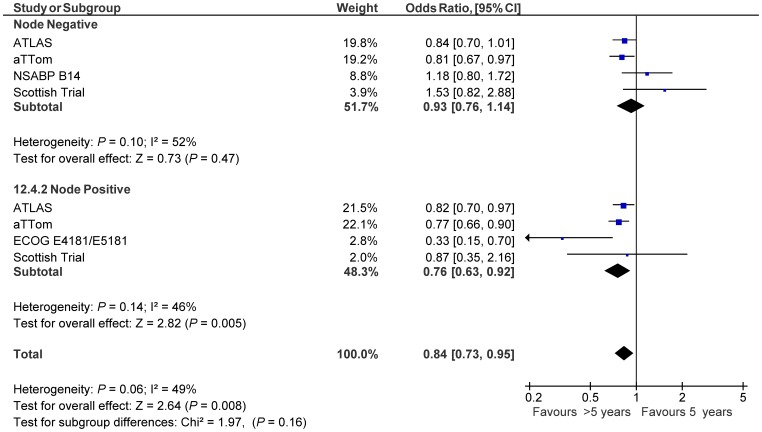
Results: Five trials comprising 21,554 patients were included. Extended adjuvant tamoxifen was not associated with a significant reduction in the risk of recurrence (OR:0.89, 95% CI 0.76-1.05, p = 0.17). There was no association between extended adjuvant tamoxifen and all-cause death (OR:0.99, 95% CI 0.84-1.16, p = 0.88). There was an apparent reduction in risk of recurrence occurring after completion of extended adjuvant tamoxifen with little evidence of effect during therapy, however, this difference was not significant (p for difference 0.10). Subgroup analysis suggested that a greater effect size among lymph node positive patients compared with those who are lymph node negative (NNT: 25 vs. 49). There was no apparent difference in the effect between pre- and post-menopausal patients. Endometrial carcinoma was substantially more frequent with extended adjuvant tamoxifen (OR:2.06, 95% CI 1.65-2.58, p<0.001, number needed to harm:89).
Conclusion: In unselected patients, extended adjuvant tamoxifen is not associated with a significant reduction in recurrence, or a reduction in all-cause death. Patients with lymph node positive breast cancer may derive some benefit. Reduction in the risk of recurrence appears to occur only after completion of extended adjuvant therapy.
Conflict of interest statement
Figures
Similar articles
-
Tamoxifen for early breast cancer: an overview of the randomised trials. Early Breast Cancer Trialists' Collaborative Group.Lancet. 1998 May 16;351(9114):1451-67. Lancet. 1998. PMID: 9605801
-
Reducing the risk for breast cancer recurrence after completion of tamoxifen treatment in postmenopausal women.Clin Ther. 2007 Aug;29(8):1535-47. doi: 10.1016/j.clinthera.2007.08.013. Clin Ther. 2007. PMID: 17919537 Review.
-
Extended adjuvant endocrine therapy in early breast cancer: a meta-analysis of published randomized trials.Med Oncol. 2017 Jul;34(7):131. doi: 10.1007/s12032-017-0986-2. Epub 2017 Jun 15. Med Oncol. 2017. PMID: 28620883
-
Patients with early stage invasive cancer with close or positive margins treated with conservative surgery and radiation have an increased risk of breast recurrence that is delayed by adjuvant systemic therapy.Int J Radiat Oncol Biol Phys. 1999 Jul 15;44(5):1005-15. doi: 10.1016/s0360-3016(99)00112-1. Int J Radiat Oncol Biol Phys. 1999. PMID: 10421533
-
Efficacy and toxicity of extended aromatase inhibitors after adjuvant aromatase inhibitors-containing therapy for hormone-receptor-positive breast cancer: a literature-based meta-analysis of randomized trials.Breast Cancer Res Treat. 2020 Jan;179(2):275-285. doi: 10.1007/s10549-019-05464-w. Epub 2019 Oct 12. Breast Cancer Res Treat. 2020. PMID: 31606823 Review.
Cited by
-
Association of tamoxifen with meningioma: a population-based study in Sweden.Eur J Cancer Prev. 2016 Jan;25(1):29-33. doi: 10.1097/CEJ.0000000000000133. Eur J Cancer Prev. 2016. PMID: 25642792 Free PMC article.
-
Factors associated with late recurrence after completion of 5-year adjuvant tamoxifen in estrogen receptor positive breast cancer.BMC Cancer. 2016 Jul 7;16:430. doi: 10.1186/s12885-016-2423-x. BMC Cancer. 2016. PMID: 27388210 Free PMC article.
-
Assessment of compliance with hormonal therapy in early breast cancer patients with positive hormone receptor phenotype: A single institution study.Breast. 2022 Apr;62:69-74. doi: 10.1016/j.breast.2022.01.017. Epub 2022 Feb 1. Breast. 2022. PMID: 35131645 Free PMC article.
-
hsa-mir-483-3p modulates delayed breast cancer recurrence.Sci Rep. 2025 Jan 3;15(1):693. doi: 10.1038/s41598-024-84437-6. Sci Rep. 2025. PMID: 39753688 Free PMC article.
-
Cancer progression and the invisible phase of metastatic colonization.Nat Rev Cancer. 2020 Nov;20(11):681-694. doi: 10.1038/s41568-020-00300-6. Epub 2020 Oct 6. Nat Rev Cancer. 2020. PMID: 33024261 Review.
References
-
- Goss PE, Ingle JN, Martino S, Robert NJ, Muss HB, et al. (2005) Randomized trial of letrozole following tamoxifen as extended adjuvant therapy in receptor-positive breast cancer: updated findings from NCIC CTG MA.17. J Natl Cancer Inst 97: 1262–1271. - PubMed
-
- Jakesz R, Greil R, Gnant M, Schmid M, Kwasny W, et al. (2007) Extended adjuvant therapy with anastrozole among postmenopausal breast cancer patients: results from the randomized Austrian Breast and Colorectal Cancer Study Group Trial 6a. J Natl Cancer Inst 99: 1845–1853. - PubMed
-
- Mamounas EP, Jeong JH, Wickerham DL, Smith RE, Ganz PA, et al. (2008) Benefit from exemestane as extended adjuvant therapy after 5 years of adjuvant tamoxifen: intention-to-treat analysis of the National Surgical Adjuvant Breast And Bowel Project B-33 trial. J Clin Oncol 26: 1965–1971. - PubMed
-
- Fisher B, Dignam J, Bryant J, Wolmark N (2001) Five versus more than five years of tamoxifen for lymph node-negative breast cancer: updated findings from the National Surgical Adjuvant Breast and Bowel Project B-14 randomized trial. J Natl Cancer Inst 93: 684–690. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
