

Comparison of efficacy of intensive versus mild pitavastatin therapy on lipid and inflammation biomarkers in hypertensive patients with dyslipidemia
- PMID: 24586502
- PMCID: PMC3929641
- DOI: 10.1371/journal.pone.0089057
Comparison of efficacy of intensive versus mild pitavastatin therapy on lipid and inflammation biomarkers in hypertensive patients with dyslipidemia
Abstract
Objective: Intensive as compared to mild statin therapy has been proven to be superior in improving cardiovascular outcome, whereas the effects of intensive statin therapy on inflammation and lipoprotein biomarkers are not well defined.
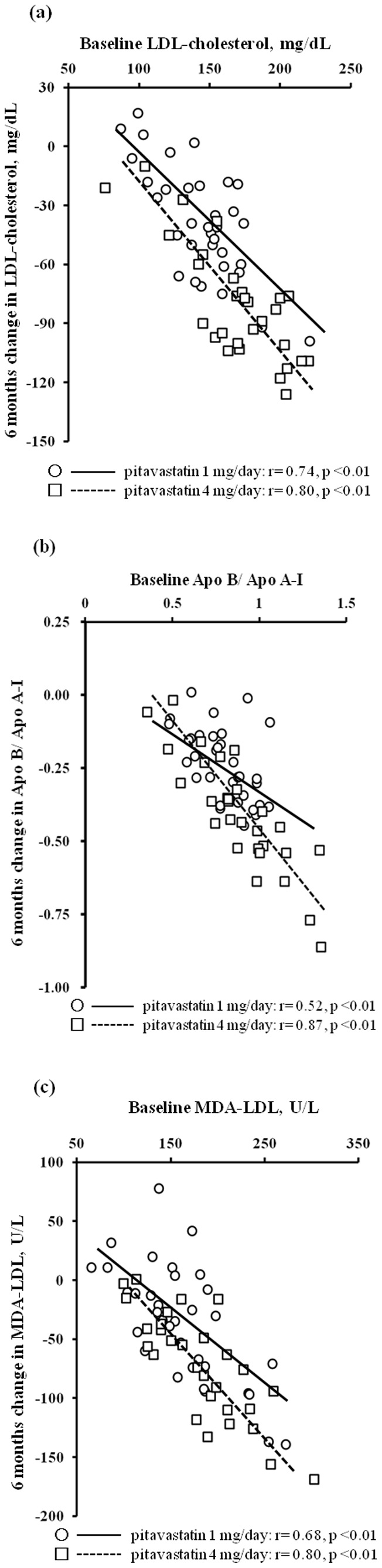
Methods: This study assigned essential hypertensive patients with dyslipidemia to 6 months administration of mild (1 mg/day, n = 34) or intensive pitavastatin therapy (4 mg/day, n = 29), and various lipid and inflammation biomarkers were measured at baseline, and 3 and 6 months after the start of treatment.
Results: Both pitavastatin doses were well tolerated, and there were no serious treatment-related adverse events. After 6 months, significant improvements in total cholesterol, triglycerides, low-density lipoprotein (LDL-) cholesterol, LDL/high-density lipoprotein cholesterol (LDL/HDL), apolipoproteins B, C-II, and E, apolipoprotein-B/apolipoprotein-A-I (Apo B/Apo A-I), and malondialdehyde (MDA-) LDL were observed in both groups. Compared with the mild pitavastatin group, the intensive pitavastatin therapy showed significantly greater decreases in C reactive protein (F = 3.76, p<0.05), total cholesterol (F = 10.65), LDL-cholesterol (F = 23.37), LDL/HDL (F = 12.34), apolipoproteins B (F = 19.07) and E (F = 6.49), Apo B/Apo A-I (F = 13.26), and MDA-LDL (F = 5.76) (p<0.01, respectively).
Conclusion: Intensive pitavastatin therapy may have a more favorable effect not only in decreasing LDL-cholesterol but also in pleiotropic benefits in terms of improvement of apolipoproteins, inflammation, or oxidation.
Conflict of interest statement
Figures
References
-
- Zanchetti A (1994) Hyperlipidemia in the hypertensive patient. Am J Med 96: 3S–8S. - PubMed
-
- Kannel WB (2000) Risk stratification in hypertension: new insights from the Framingham Study. Am J Hypertens 13: 3S–10S. - PubMed
-
- Selby JV, Peng T, Karter AJ, Alexander M, Sidney S, et al. (2004) High rates of co-occurrence of hypertension, elevated low-density lipoprotein cholesterol, and diabetes mellitus in a large managed care population. Am J Manag Care 10: 163–170. - PubMed
-
- Sever PS, Dahlof B, Poulter NR, Wedel H, Beevers G, et al. (2003) Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial–Lipid Lowering Arm (ASCOT-LLA): a multicentre randomised controlled trial. Lancet 361: 1149–1158. - PubMed
-
- Ridker PM, Danielson E, Fonseca FA, Genest J, Gotto AM Jr, et al. (2008) Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med 359: 2195–2207. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
