

Effects of physician-nurse substitution on clinical parameters: a systematic review and meta-analysis
- PMID: 24586577
- PMCID: PMC3933531
- DOI: 10.1371/journal.pone.0089181
Effects of physician-nurse substitution on clinical parameters: a systematic review and meta-analysis
Abstract
Background: Physicians' shortage in many countries and demands of high-quality and affordable care make physician-nurse substitution an appealing workforce strategy. The objective of this study is to conduct a systematic review and meta-analysis of randomised controlled trials (RCTs) assessing the impact of physician-nurse substitution in primary care on clinical parameters.
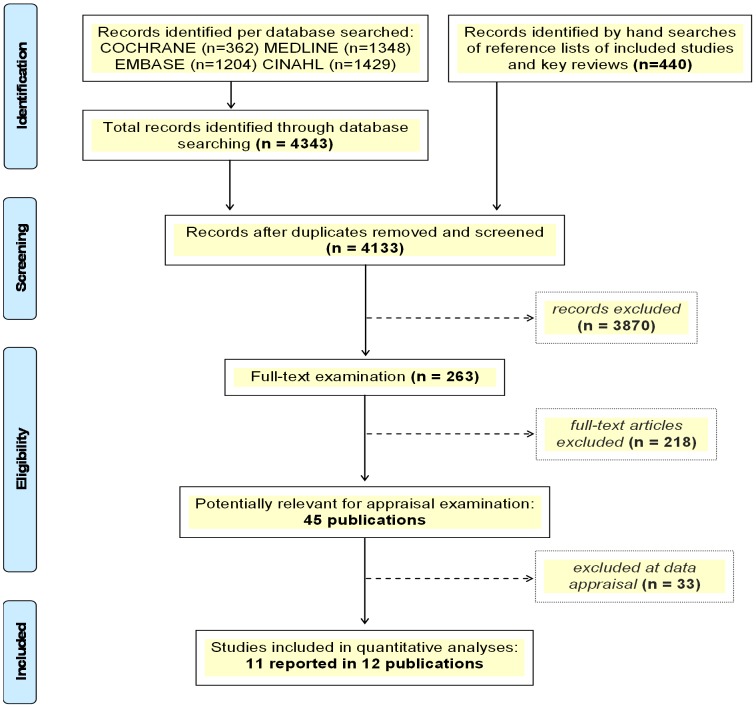
Methods: We systematically searched OVID Medline and Embase, The Cochrane Library and CINAHL, up to August 2012; selected peer-reviewed RCTs comparing physician-led care with nurse-led care on changes in clinical parameters. Study selection and data extraction were performed in duplicate by independent reviewers. We assessed the individual study risk of bias; calculated the study-specific and pooled relative risks (RR) or weighted mean differences (WMD); and performed fixed-effects meta-analyses.
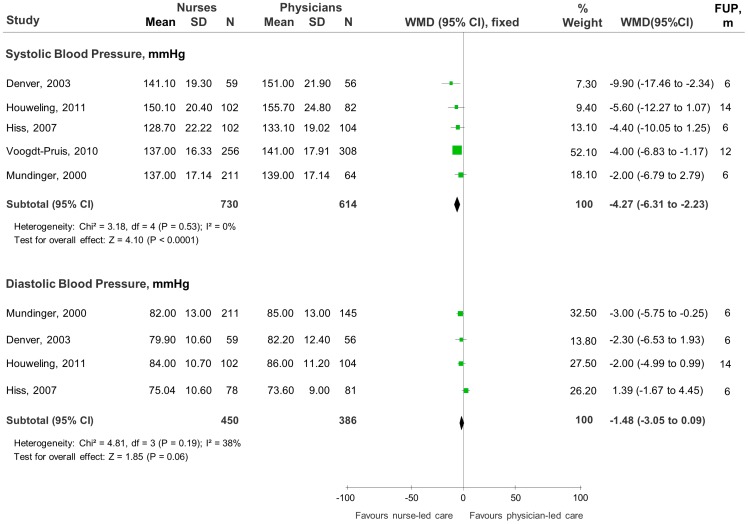
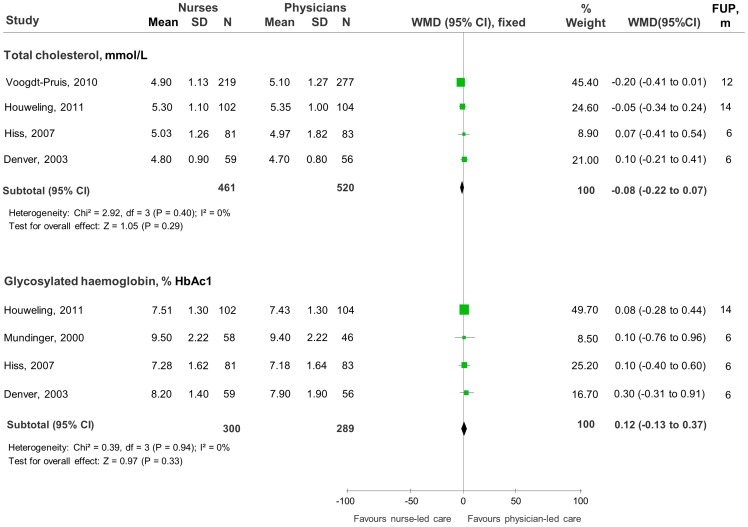
Results: 11 RCTs (N = 30,247) were included; most were from Europe, generally small with higher risk of bias. In all studies, nurses provided care for complex conditions including HIV, hypertension, heart failure, cerebrovascular diseases, diabetes, asthma, Parkinson's disease and incontinence. Meta-analyses showed greater reductions in systolic blood pressure (SBP) in favour of nurse-led care (WMD -4.27 mmHg, 95% CI -6.31 to -2.23) but no statistically significant differences between groups in the reduction of diastolic blood pressure (DBP) (WMD -1.48 mmHg, 95%CI -3.05 to -0.09), total cholesterol (TC) (WMD -0.08 mmol/l, 95%CI -0.22 to 0.07) or glycosylated haemoglobin (WMD 0.12%HbAc1, 95%CI -0.13 to 0.37). Of other 32 clinical parameters identified, less than a fifth favoured nurse-led care while 25 showed no significant differences between groups.
Limitations: disease-specific interventions from a small selection of healthcare systems, insufficient quantity and quality of studies, many different parameters.
Conclusions: trained nurses appeared to be better than physicians at lowering SBP but similar at lowering DBP, TC or HbA1c. There is insufficient evidence that nurse-led care leads to better outcomes of other clinical parameters than physician-led care.
Conflict of interest statement
Figures
References
-
- WHO (2006) The world health report: working together for health. Geneva, Switzerland: World Health Organization.
-
- WHO (2008) Task shifting: rational redistribution of tasks among health workforce teams: global recommendations and guidelines. Geneva, Switzerland: World Health Organization.
-
- WHO (2012) World Health Statistics 2012: Indicator compendium. Geneva, Switzerland: World Health Organization.
-
- Salsberg E, Grover A (2006) Physician workforce shortages: implications and issues for academic health centers and policymakers. Acad Med 81: 782–7. - PubMed
-
- Sibbald B, Shen J, McBride A (2004) Changing the skill-mix of the health care workforce. J Health Serv Res Policy 9(1): S28–38. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
