

Changes in nephritogenic serum galactose-deficient IgA1 in IgA nephropathy following tonsillectomy and steroid therapy
- PMID: 24586974
- PMCID: PMC3931817
- DOI: 10.1371/journal.pone.0089707
Changes in nephritogenic serum galactose-deficient IgA1 in IgA nephropathy following tonsillectomy and steroid therapy
Abstract
Background: Recent studies have shown that galactose-deficient IgA1 (GdIgA1) has an important role in the pathogenesis of IgA nephropathy (IgAN). Although emerging data suggest that serum GdIgA1 can be a useful non-invasive IgAN biomarker, the localization of nephritogenic GdIgA1-producing B cells remains unclear. Recent clinical and experimental studies indicate that immune activation tonsillar toll-like receptor (TLR) 9 may be involved in the pathogenesis of IgAN. Here we assessed the possibility of GdIgA1 production in the palatine tonsils in IgAN patients.
Methods: We assessed changes in serum GdIgA1 levels in IgAN patients with clinical remission of hematuria and proteinuria following combined tonsillectomy and steroid pulse therapy. Further, the association between clinical outcome and tonsillar TLR9 expression was evaluated.
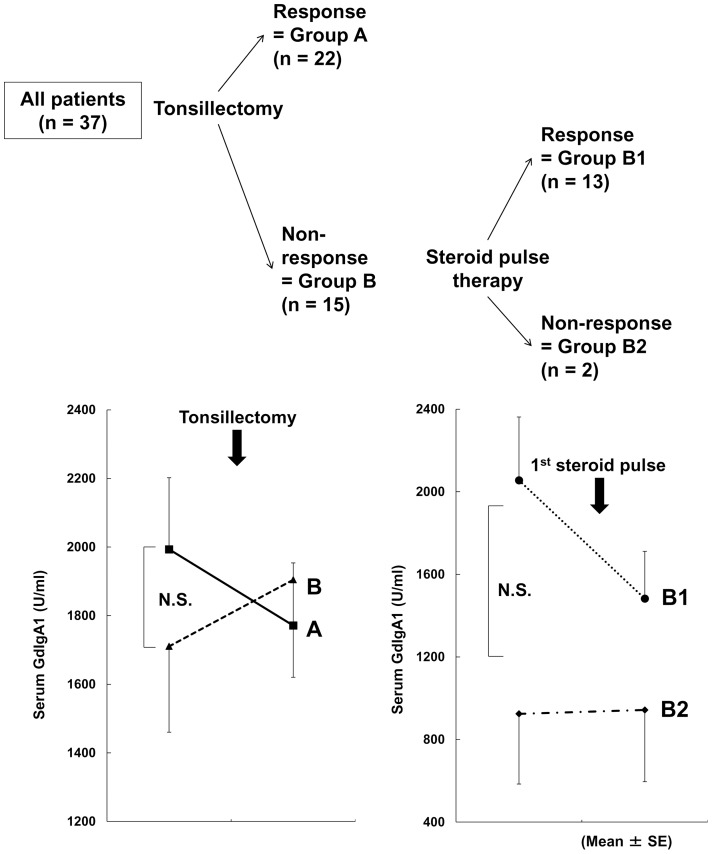
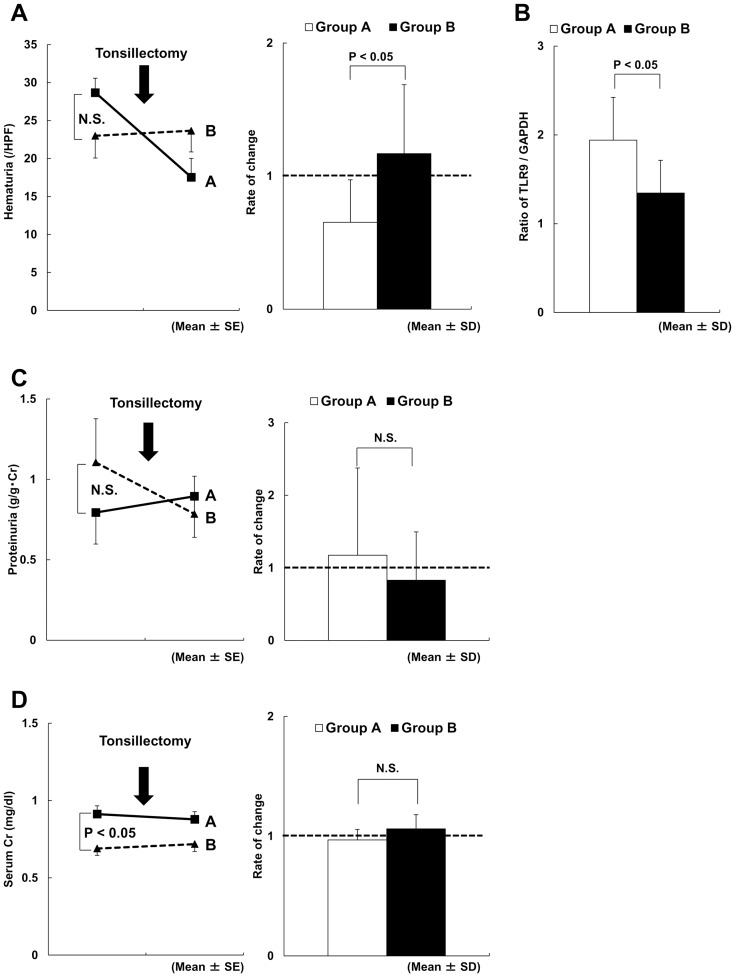
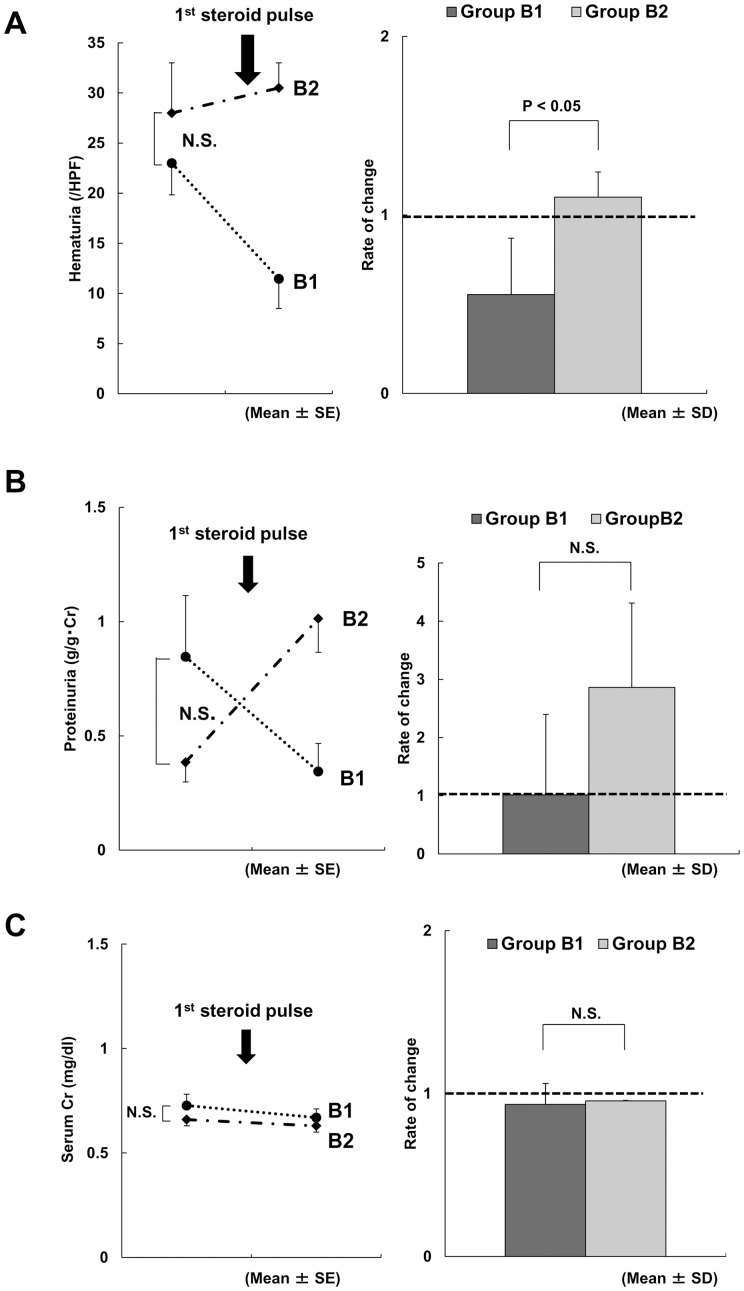
Results: Patients (n = 37) were divided into two groups according to therapy response. In one group, serum GdIgA1 levels decreased after tonsillectomy (59%) alone, whereas in the other group most levels only decreased after the addition of steroid pulse therapy to tonsillectomy (41%). The former group showed significantly higher tonsillar TLR9 expression and better improvement in hematuria immediately after tonsillectomy than the latter group.
Conclusions: The present study indicates that the palatine tonsils are probably a major sites of GdIgA1-producing cells. However, in some patients these cells may propagate to other lymphoid organs, which may partially explain the different responses observed to tonsillectomy alone. These findings help to clarify some of the clinical observations in the management of IgAN, and may highlight future directions for research.
Conflict of interest statement
Figures
References
-
- Berger J, Hinglais N (1968) Les Depots intercapillaries d'IgA-IgG. J Urol Nephrol 74: 694–695. - PubMed
-
- Cuevas X, Lloveras J, Mir M, Aubia J, Masramon J (1987) Disappearance of mesangial IgA deposits from the kidney of two donors after transplantation. Transplant Proc 19: 2208–2209. - PubMed
-
- Sanfilippo F, Croker BP, Bollinger RR (1982) Fate of four cadaveric donor renal allografts with mesangial IgA deposits. Transplantation 33: 370–376. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
