

Features on MDCT that predict surgery in patients with adhesive-related small bowel obstruction
- PMID: 24587047
- PMCID: PMC3933662
- DOI: 10.1371/journal.pone.0089804
Features on MDCT that predict surgery in patients with adhesive-related small bowel obstruction
Abstract
Purpose: The purpose of this study was to determine the contribution of multidetector-row computed tomography (MDCT) in the management of adhesion-related small bowel obstruction (SBO) and to identify its predictive value for surgery.
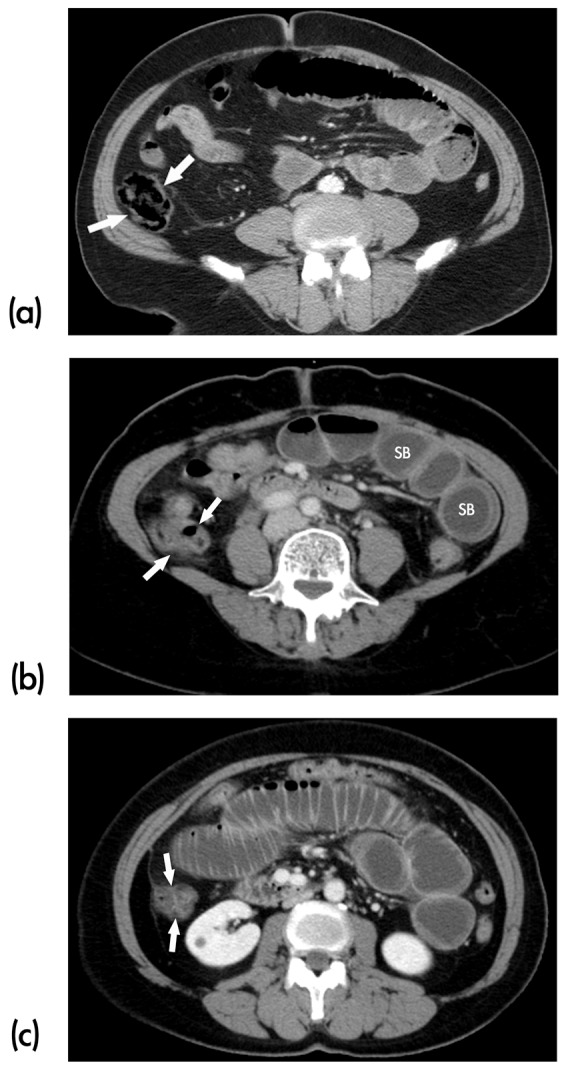
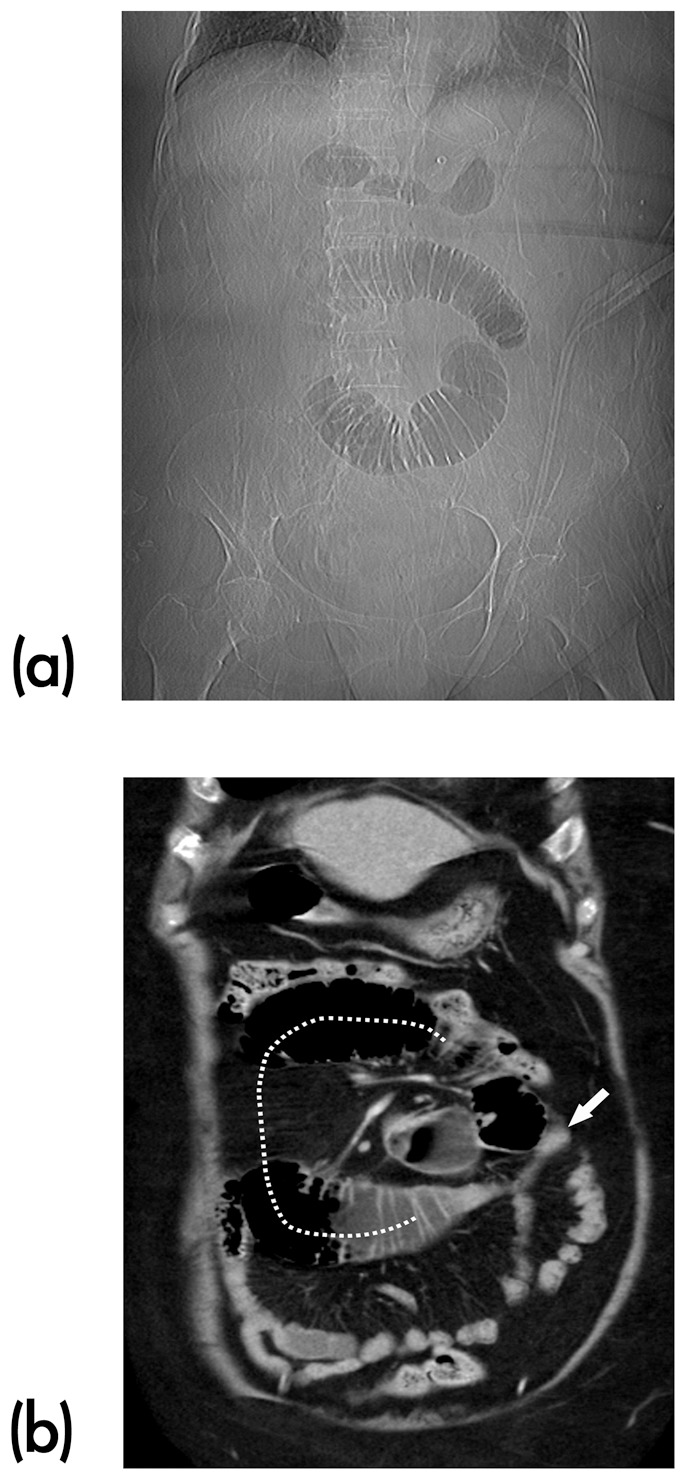
Methods: We conducted a retrospective review of 151 patients over a 5-year period with the diagnosis of SBO caused by adhesion. These patients were divided into two groups: surgery (n = 63) and observation group (n = 88). Two radiologists blinded to the outcome of the patients evaluated MDCT images retrospectively, recording the bowel diameter, bowel wall thickness, degree of obstruction, air-fluid level, mesenteric fatty stranding, transitional zone, intraperitoneal fluid, close loop, whirl sign, and faeces sign. Statistical analyses were performed using univariate and multivariable analyses.
Results: Multivariable analysis showed that MDCT demonstrated presence of intraperitoneal fluid (Odds ratio, OR, 4.38), high-grade or complete obstruction (OR, 3.19) and mesenteric fatty stranding (OR, 2.81), and absence of faeces sign (OR, 2.11) were the most significant predictors. When all of the four criteria were used in combination, high sensitivity of 98.4% and specificity of 90.9% were achieved for the prediction for surgery.
Conclusion: MDCT is useful to evaluate adhesion-related SBO and to predict accurately patients who require surgery. Use of the four MDCT features in combination is highly suggestive of the need for early surgical intervention.
Conflict of interest statement
Figures


Similar articles
-
Imaging differentiation of phytobezoar and small-bowel faeces: CT characteristics with quantitative analysis in patients with small- bowel obstruction.Eur Radiol. 2015 Apr;25(4):922-31. doi: 10.1007/s00330-014-3486-1. Epub 2014 Nov 23. Eur Radiol. 2015. PMID: 25417124
-
Small bowel obstruction-who needs an operation? A multivariate prediction model.World J Surg. 2010 May;34(5):910-9. doi: 10.1007/s00268-010-0479-3. World J Surg. 2010. PMID: 20217412 Free PMC article.
-
Value of MDCT and Clinical and Laboratory Data for Predicting the Need for Surgical Intervention in Suspected Small-Bowel Obstruction.AJR Am J Roentgenol. 2017 Apr;208(4):785-793. doi: 10.2214/AJR.16.16946. AJR Am J Roentgenol. 2017. PMID: 28328258
-
MDCT findings in small bowel obstruction: implications of the cause and presence of complications on treatment decisions.Abdom Imaging. 2015 Oct;40(7):2248-62. doi: 10.1007/s00261-015-0477-x. Abdom Imaging. 2015. PMID: 26070748 Review.
-
Adhesive Small Bowel Obstruction: Predictive Radiology to Improve Patient Management.Radiology. 2020 Sep;296(3):480-492. doi: 10.1148/radiol.2020192234. Epub 2020 Jul 21. Radiology. 2020. PMID: 32692296 Review.
Cited by
-
Vascular assessment in small bowel obstruction: can CT predict requirement for surgical intervention?Abdom Radiol (NY). 2021 Feb;46(2):517-525. doi: 10.1007/s00261-020-02698-x. Epub 2020 Aug 8. Abdom Radiol (NY). 2021. PMID: 32770400
-
Increased unenhanced bowel-wall attenuation: a specific sign of bowel necrosis in closed-loop small-bowel obstruction.Eur Radiol. 2018 Oct;28(10):4225-4233. doi: 10.1007/s00330-018-5402-6. Epub 2018 Apr 20. Eur Radiol. 2018. PMID: 29679213
-
Development and external validation of prediction risk scores (STRISK and NOFA) to predict immediate surgical need in adhesive small bowel obstruction: an observational prospective multicentre study.Br J Surg. 2025 Mar 4;112(3):znaf025. doi: 10.1093/bjs/znaf025. Br J Surg. 2025. PMID: 40105480 Free PMC article.
-
Diagnostic utility of CT for small bowel obstruction: Systematic review and meta-analysis.PLoS One. 2019 Dec 30;14(12):e0226740. doi: 10.1371/journal.pone.0226740. eCollection 2019. PLoS One. 2019. PMID: 31887146 Free PMC article.
-
Prognostic factors to identify resolution of small bowel obstruction without need for operative management: systematic review.Eur Radiol. 2024 Jun;34(6):3861-3871. doi: 10.1007/s00330-023-10421-9. Epub 2023 Nov 8. Eur Radiol. 2024. PMID: 37938387 Free PMC article.
References
-
- Foster NM, MCGory ML, Zingmond DS, Ko CY (2006) Small bowel obstruction: a population-based appraisal. J Am Coll Surg 203: 170–176. - PubMed
-
- Petrovic B, Nikolaidis P, Hammond NA, Grant TH, Miller FH (2006) Identification of adhesions on CT in small-bowel obstruction. Emerg Radiol 12: 88–93. - PubMed
-
- Hwang JY, Lee JK, Lee JE, Baek SY (2009) Value of multidetector CT in decision making regarding surgery in patients with small-bowel obstruction due to adhesion. Eur Radiol 19: 2425–2431. - PubMed
-
- Jones K, Mangram AJ, Lebron RA, Nadalo L, Dunn E (2007) Can a computed tomography scoring system predict the need for surgery in small-bowel obstruction? Am J Surg 194: 780–783. - PubMed
-
- Taourel PG, Fabre JM, Pradel JA, Seneterre EJ, Megibow AJ, et al. (1995) Value of CT in the diagnosis and management of patients with suspected acute small-bowel obstruction. Am J Roentgenol 165: 1187–1192. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
