

Hospital presenting self-harm and risk of fatal and non-fatal repetition: systematic review and meta-analysis
- PMID: 24587141
- PMCID: PMC3938547
- DOI: 10.1371/journal.pone.0089944
Hospital presenting self-harm and risk of fatal and non-fatal repetition: systematic review and meta-analysis
Abstract
Background: Non-fatal self-harm is one of the most frequent reasons for emergency hospital admission and the strongest risk factor for subsequent suicide. Repeat self-harm and suicide are key clinical outcomes of the hospital management of self-harm. We have undertaken a comprehensive review of the international literature on the incidence of fatal and non-fatal repeat self-harm and investigated factors influencing variation in these estimates as well as changes in the incidence of repeat self-harm and suicide over the last 30 years.
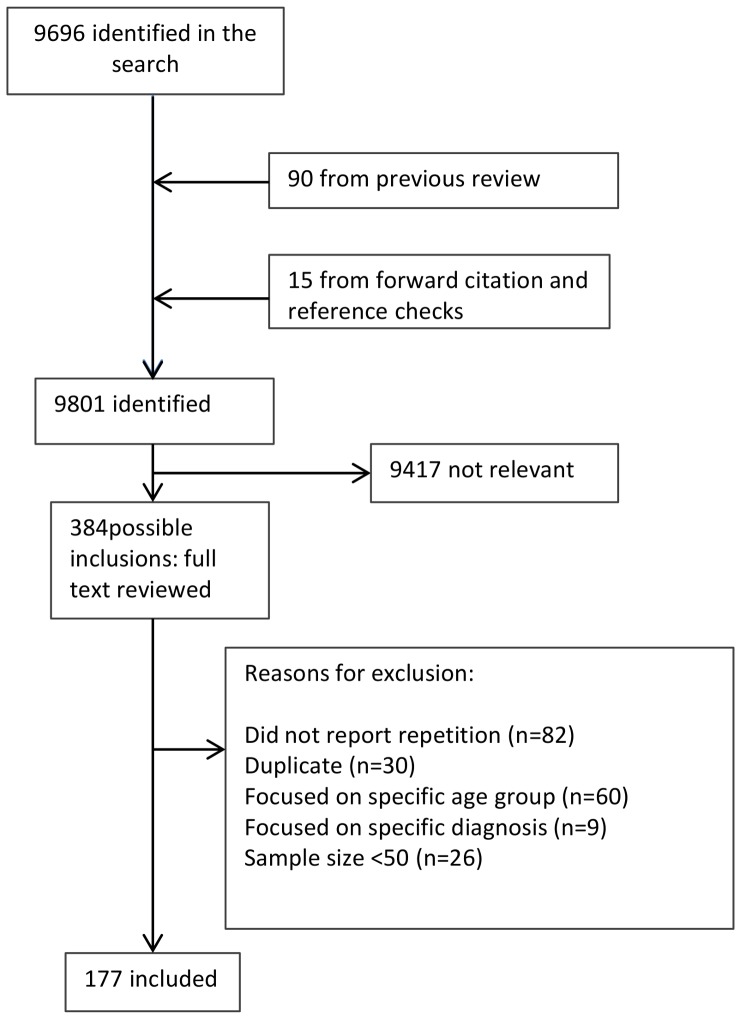
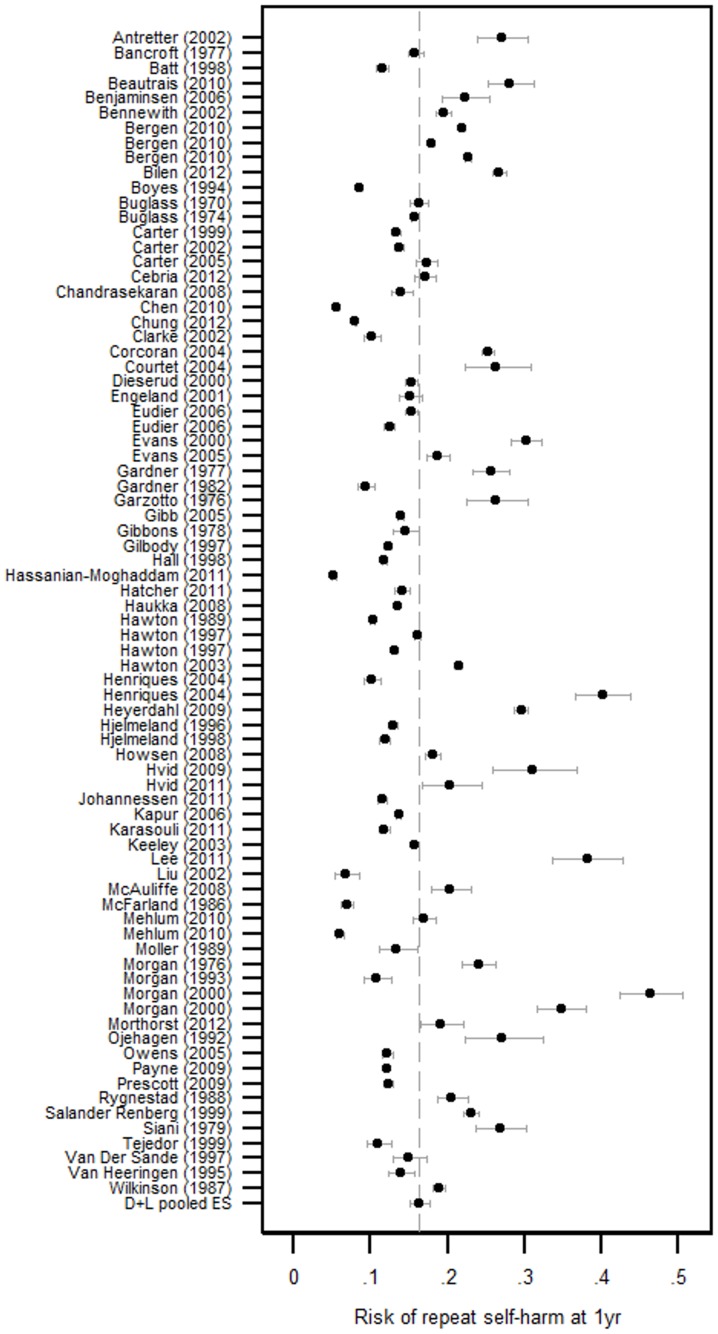
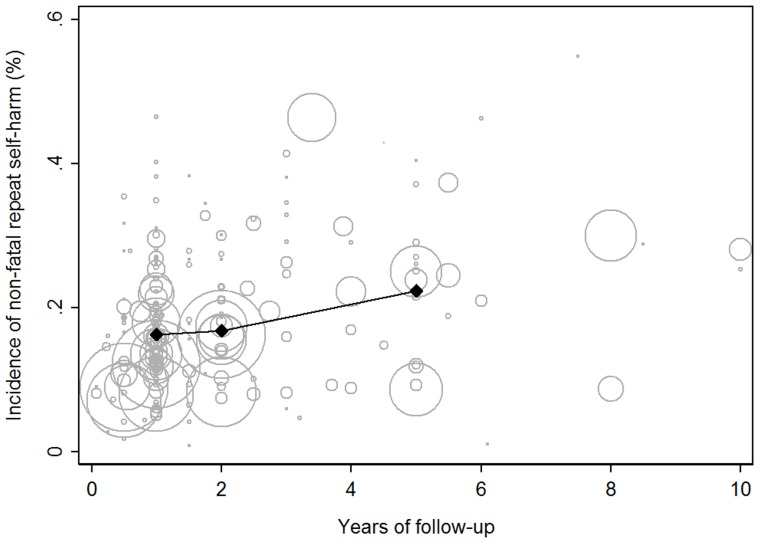
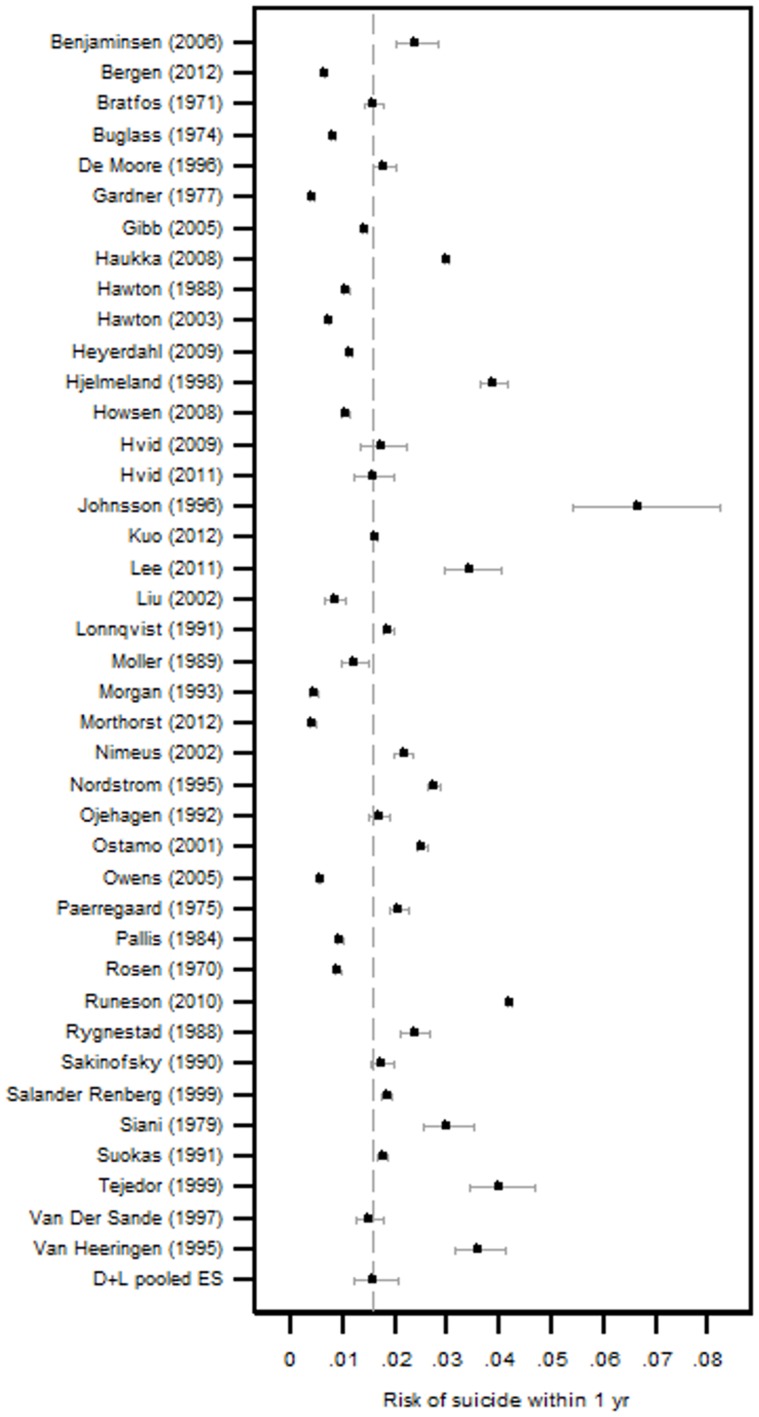
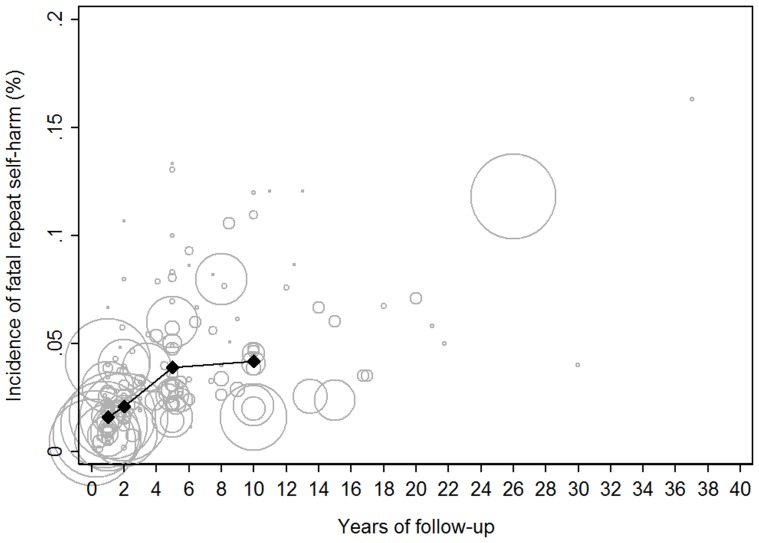
Methods and findings: Medline, EMBASE, PsycINFO, Google Scholar, article reference lists and personal paper collections of the authors were searched for studies describing rates of fatal and non-fatal self-harm amongst people who presented to health care services for deliberate self-harm. Heterogeneity in pooled estimates of repeat self-harm incidence was investigated using stratified meta-analysis and meta-regression. The search identified 177 relevant papers. The risk of suicide in the 12 months after an index attempt was 1.6% (CI 1.2-2.4) and 3.9% (CI 3.2-4.8) after 5 years. The estimated 1 year rate of non-fatal repeat self-harm was 16.3% (CI 15.1-17.7). This proportion was considerably lower in Asian countries (10.0%, CI 7.3-13.6%) and varies between studies identifying repeat episodes using hospital admission data (13.7%, CI 12.3-15.3) and studies using patient report (21.9%, CI 14.3-32.2). There was no evidence that the incidence of repeat self-harm was lower in more recent (post 2000) studies compared to those from the 1980s and 1990s.
Conclusions: One in 25 patients presenting to hospital for self-harm will kill themselves in the next 5 years. The incidence of repeat self-harm and suicide in this population has not changed in over 10 years. Different methods of identifying repeat episodes of self-harm produce varying estimates of incidence and this heterogeneity should be considered when evaluating interventions aimed at reducing non-fatal repeat self-harm.
Conflict of interest statement
Figures
References
-
- Foster T, Gillespie K, McClelland R, Patterson C (1999) Risk factors for suicide independent of DSM-III-R Axis I disorder. Case-control psychological autopsy study in Northern Ireland. Br J Psychiatry 175: 175–179. - PubMed
-
- Gairin I, House A, Owens D (2003) Attendance at the accident and emergency department in the year before suicide: retrospective study. Br J Psychiatry 183: 28–33. - PubMed
-
- Hawton K, Zahl D, Weatherall R (2003) Suicide following deliberate self-harm: long-term follow-up of patients who presented to a general hospital. Br J Psychiatry 182: 537–542. - PubMed
-
- Sinclair JM, Gray A, Rivero-Arias O, Saunders KE, Hawton K (2011) Healthcare and social services resource use and costs of self-harm patients. Soc Psychiatry Psychiatr Epidemiol 46: 263–271. - PubMed
-
- Zahl DL, Hawton K (2004) Repetition of deliberate self-harm and subsequent suicide risk: long-term follow-up study of 11,583 patients. Br J Psychiatry 185: 70–75. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
