

Conditioned pain modulation and situational pain catastrophizing as preoperative predictors of pain following chest wall surgery: a prospective observational cohort study
- PMID: 24587268
- PMCID: PMC3935997
- DOI: 10.1371/journal.pone.0090185
Conditioned pain modulation and situational pain catastrophizing as preoperative predictors of pain following chest wall surgery: a prospective observational cohort study
Abstract
Background: Variability in patients' postoperative pain experience and response to treatment challenges effective pain management. Variability in pain reflects individual differences in inhibitory pain modulation and psychological sensitivity, which in turn may be clinically relevant for the disposition to acquire pain. The aim of this study was to investigate the effects of conditioned pain modulation and situational pain catastrophizing on postoperative pain and pain persistency.
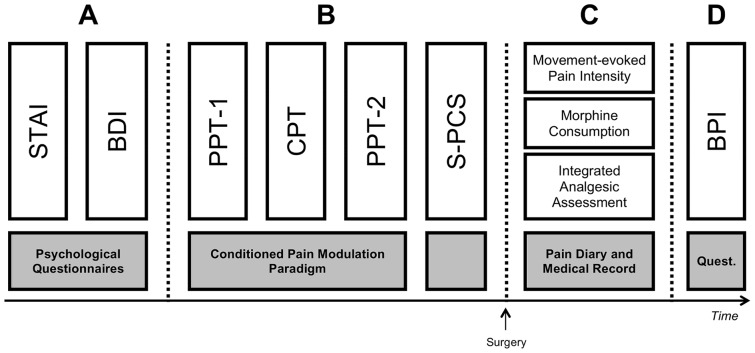
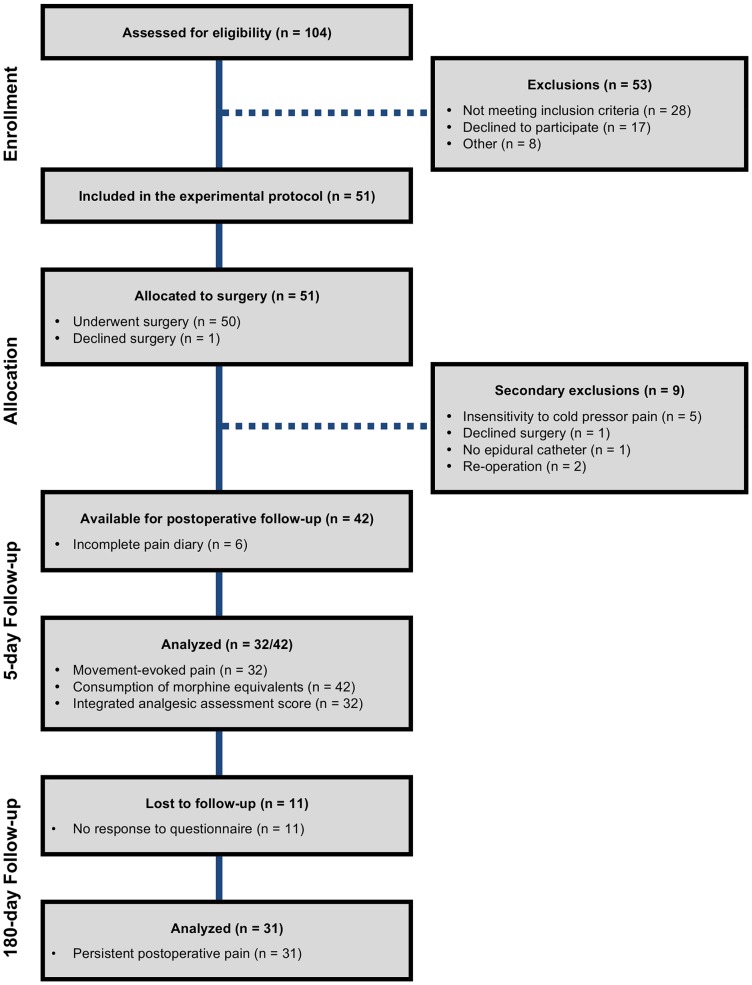
Methods: Preoperatively, 42 healthy males undergoing funnel chest surgery completed the Spielberger's State-Trait Anxiety Inventory and Beck's Depression Inventory before undergoing a sequential conditioned pain modulation paradigm. Subsequently, the Pain Catastrophizing Scale was introduced and patients were instructed to reference the conditioning pain while answering. Ratings of movement-evoked pain and consumption of morphine equivalents were obtained during postoperative days 2-5. Pain was reevaluated at six months postoperatively.
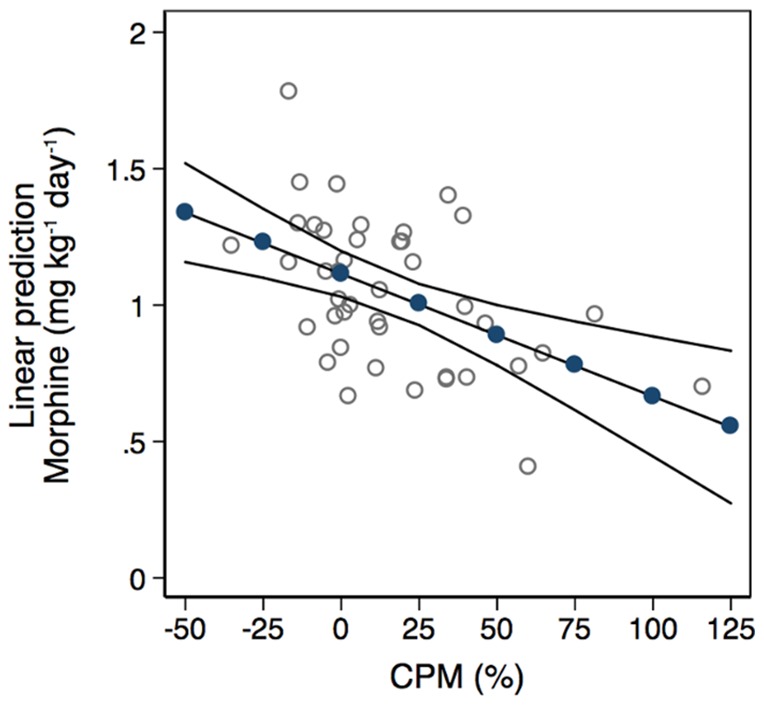
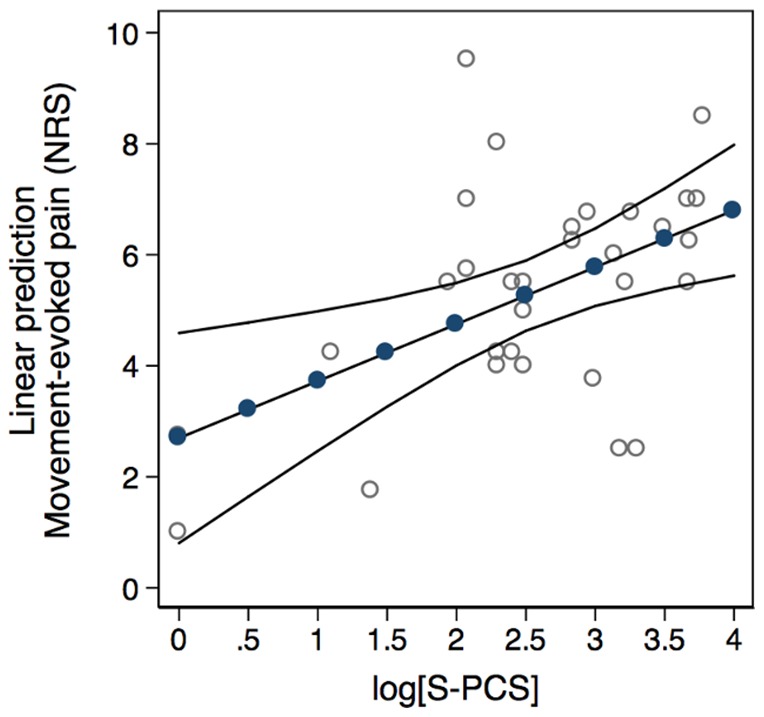
Results: Patients reporting persistent pain at six months follow-up (n = 15) were not significantly different from pain-free patients (n = 16) concerning preoperative conditioned pain modulation response (Z = 1.0, P = 0.3) or level of catastrophizing (Z = 0.4, P = 1.0). In the acute postoperative phase, situational pain catastrophizing predicted movement-evoked pain, independently of anxiety and depression (β = 1.0, P = 0.007) whereas conditioned pain modulation predicted morphine consumption (β = -0.005, P = 0.001).
Conclusions: Preoperative conditioned pain modulation and situational pain catastrophizing were not associated with the development of persistent postoperative pain following funnel chest repair. Secondary outcome analyses indicated that conditioned pain modulation predicted morphine consumption and situational pain catastrophizing predicted movement-evoked pain intensity in the acute postoperative phase. These findings may have important implications for developing strategies to treat or prevent acute postoperative pain in selected patients. Pain may be predicted and the malfunctioning pain inhibition mechanism as tested with CPM may be treated with suitable drugs augmenting descending inhibition.
Conflict of interest statement
Figures
Similar articles
-
Situational but Not Dispositional Pain Catastrophizing Correlates With Early Postoperative Pain in Pain-Free Patients Before Surgery.J Pain. 2016 May;17(5):549-60. doi: 10.1016/j.jpain.2015.12.016. Epub 2016 Jan 6. J Pain. 2016. PMID: 26772418
-
Preoperative pain catastrophizing and postoperative pain after total knee arthroplasty: a prospective cohort study with one year follow-up.BMC Musculoskelet Disord. 2016 May 17;17:214. doi: 10.1186/s12891-016-1073-0. BMC Musculoskelet Disord. 2016. PMID: 27188877 Free PMC article.
-
Associations between postoperative analgesic consumption and distress tolerance, anxiety, depression, and pain catastrophizing: a prospective observational study.Braz J Anesthesiol. 2022 Sep-Oct;72(5):567-573. doi: 10.1016/j.bjane.2021.07.007. Epub 2021 Aug 4. Braz J Anesthesiol. 2022. PMID: 34363820 Free PMC article.
-
Psychological Factors and Conditioned Pain Modulation: A Meta-Analysis.Clin J Pain. 2016 Jun;32(6):541-54. doi: 10.1097/AJP.0000000000000296. Clin J Pain. 2016. PMID: 26340657 Review.
-
Assessment of conditioned pain modulation in healthy participants and patients with chronic pain: manifestations and implications for pain progression.Curr Opin Support Palliat Care. 2019 Jun;13(2):99-106. doi: 10.1097/SPC.0000000000000419. Curr Opin Support Palliat Care. 2019. PMID: 30855554 Review.
Cited by
-
Disease-Related, Nondisease-Related, and Situational Catastrophizing in Sickle Cell Disease and Its Relationship With Pain.J Pain. 2016 Nov;17(11):1227-1236. doi: 10.1016/j.jpain.2016.08.003. Epub 2016 Aug 20. J Pain. 2016. PMID: 27555427 Free PMC article.
-
Short-term test-retest-reliability of conditioned pain modulation using the cold-heat-pain method in healthy subjects and its correlation to parameters of standardized quantitative sensory testing.BMC Neurol. 2016 Aug 5;16:125. doi: 10.1186/s12883-016-0650-z. BMC Neurol. 2016. PMID: 27495743 Free PMC article.
-
Development and Validation of a Predictive Model of Pain Modulation Profile to Guide Chronic Pain Treatment: A Study Protocol.Front Pain Res (Lausanne). 2021 Feb 15;2:606422. doi: 10.3389/fpain.2021.606422. eCollection 2021. Front Pain Res (Lausanne). 2021. PMID: 35295452 Free PMC article.
-
Ultrasound-guided bilateral quadratus lumborum block vs. intrathecal morphine for postoperative analgesia after cesarean section: a randomized controlled trial.Korean J Anesthesiol. 2020 Apr;73(2):121-128. doi: 10.4097/kja.d.18.00269. Epub 2019 Mar 8. Korean J Anesthesiol. 2020. PMID: 30852882 Free PMC article. Clinical Trial.
-
Pain Sensitivity and Pain Catastrophizing Are Associated With Persistent Pain and Disability After Lumbar Spine Surgery.Arch Phys Med Rehabil. 2015 Oct;96(10):1763-70. doi: 10.1016/j.apmr.2015.06.003. Epub 2015 Jun 20. Arch Phys Med Rehabil. 2015. PMID: 26101845 Free PMC article.
References
-
- White PF, Kehlet H (2010) Improving postoperative pain management: what are the unresolved issues? Anesthesiology 112: 220–225. - PubMed
-
- Apfelbaum JL, Chen C, Mehta SS, Gan TJ (2003) Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg 97: 534–540, table of contents. - PubMed
-
- Dolin SJ, Cashman JN, Bland JM (2002) Effectiveness of acute postoperative pain management: I. Evidence from published data. Br J Anaesth 89: 409–423. - PubMed
-
- Sommer M, de Rijke JM, van Kleef M, Kessels AG, Peters ML, et al. (2008) The prevalence of postoperative pain in a sample of 1490 surgical inpatients. Eur J Anaesthesiol 25: 267–274. - PubMed
-
- Moore RA, Edwards JE, McQuay HJ (2005) Acute pain: individual patient meta-analysis shows the impact of different ways of analysing and presenting results. Pain 116: 322–331. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
