

Monocytes expand with immune dysregulation and is associated with insulin resistance in older individuals with chronic HIV
- PMID: 24587328
- PMCID: PMC3937368
- DOI: 10.1371/journal.pone.0090330
Monocytes expand with immune dysregulation and is associated with insulin resistance in older individuals with chronic HIV
Abstract
Background: Rates of insulin resistance are increased in HIV-infected patients on stable antiretroviral therapy (ART). Such increase may partially be due to HIV-induced immune dysregulation involving monocytes (MO) and its subsets.
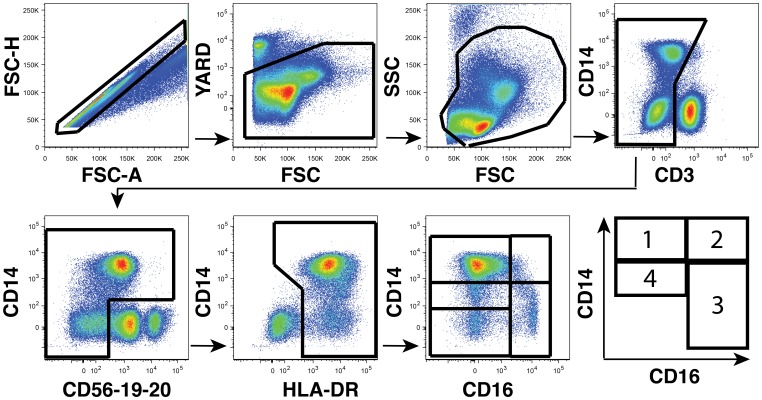
Materials and methods: Cross-sectional analysis of 141 HIV-infected subjects age ≥ 40 years on stable ART. Homeostatic model assessment-insulin resistance (HOMA-IR) and rates of metabolic syndrome were calculated. Subjects were classified by fasting glucose and oral glucose tolerance test (OGTT) into clinical diabetes categories. Multi-parametric flow cytometry was used to determine MO subset percentages: [classical (CD14(++)CD16(-)), intermediate (CD14(++)CD16(+)), non-classical (CD14(low/+)CD16(++)), and a recently identified fourth (CD14(low/+)CD16(-)) 'transitional' MO subset] and percentage of activated (CD38(+)HLA-DR(+)) CD8 T cells. Absolute levels of cells were calculated using clinical CBC and T cell subset data. Multiple plasma soluble biomarkers were assessed by Luminex technology.
Results: Median age 50 years, CD4 count (percent) 505 cells/µL (29%), and 89% male. Total MO (r=-0.23, p=0.006) and classical and non-classical MO subsets correlated negatively with CD4 percent. No correlations were seen with CD4 count as absolute values. Log-total MO and log-classical MO predicted HOMA-IR independently of HIV immuno-virologic and diabetes risk factors (β=0.42, p=0.02 and β=0.35, p=0.02, respectively) and were increased in subjects with metabolic syndrome (p=0.03 and p=0.05 respectively). Total and/or subset MO levels correlated with multiple soluble plasma biomarkers including CRP, IL-6, MMP-9, MPO, SAA, SAP and tPAI-1, with tPAI-1 independently predicting HOMA-IR (β=0.74, p<0.001).
Conclusions: MO levels increase with worsening HIV immune dysregulation as assessed by CD4 percent. CD4 percent may provide additional information about MO and metabolic risk in this population beyond absolute values. MO, and specifically classical MO, may contribute to insulin resistance and metabolic syndrome during chronic HIV infection. Multiple soluble plasma biomarkers including tPAI-1 increase with increase in MO. Levels of tPAI-1 independently predict the development of insulin resistance.
Conflict of interest statement
Figures


Similar articles
-
Non-classical monocytes predict progression of carotid artery bifurcation intima-media thickness in HIV-infected individuals on stable antiretroviral therapy.HIV Clin Trials. 2016 May;17(3):114-22. doi: 10.1080/15284336.2016.1162386. Epub 2016 Apr 4. HIV Clin Trials. 2016. PMID: 27125366 Free PMC article.
-
Monocyte Based Correlates of Immune Activation and Viremia in HIV-Infected Long-Term Non-Progressors.Front Immunol. 2019 Dec 6;10:2849. doi: 10.3389/fimmu.2019.02849. eCollection 2019. Front Immunol. 2019. PMID: 31867010 Free PMC article.
-
CD14(high)CD16(+) rather than CD14(low)CD16(+) monocytes correlate with disease progression in chronic HIV-infected patients.J Acquir Immune Defic Syndr. 2009 Dec;52(5):553-9. doi: 10.1097/qai.0b013e3181c1d4fe. J Acquir Immune Defic Syndr. 2009. PMID: 19950429
-
Glucose Metabolism in T Cells and Monocytes: New Perspectives in HIV Pathogenesis.EBioMedicine. 2016 Apr;6:31-41. doi: 10.1016/j.ebiom.2016.02.012. Epub 2016 Feb 6. EBioMedicine. 2016. PMID: 27211546 Free PMC article. Review.
-
Dysfunctional Immunometabolism in HIV Infection: Contributing Factors and Implications for Age-Related Comorbid Diseases.Curr HIV/AIDS Rep. 2020 Apr;17(2):125-137. doi: 10.1007/s11904-020-00484-4. Curr HIV/AIDS Rep. 2020. PMID: 32140979 Free PMC article. Review.
Cited by
-
T Lymphocyte Subsets Associated With Prevalent Diabetes in Veterans With and Without Human Immunodeficiency Virus.J Infect Dis. 2020 Jun 29;222(2):252-262. doi: 10.1093/infdis/jiaa069. J Infect Dis. 2020. PMID: 32052044 Free PMC article.
-
Blood monocyte and dendritic cell profiles among people living with HIV with Mycobacterium tuberculosis co-infection.BMC Immunol. 2023 Jul 21;24(1):21. doi: 10.1186/s12865-023-00558-z. BMC Immunol. 2023. PMID: 37480005 Free PMC article.
-
Non-Classical Monocytes and Monocyte Chemoattractant Protein-1 (MCP-1) Correlate with Coronary Artery Calcium Progression in Chronically HIV-1 Infected Adults on Stable Antiretroviral Therapy.PLoS One. 2016 Feb 11;11(2):e0149143. doi: 10.1371/journal.pone.0149143. eCollection 2016. PLoS One. 2016. PMID: 26867220 Free PMC article.
-
Loss of intraepidermal nerve fiber density during SIV peripheral neuropathy is mediated by monocyte activation and elevated monocyte chemotactic proteins.J Neuroinflammation. 2015 Dec 18;12:237. doi: 10.1186/s12974-015-0456-8. J Neuroinflammation. 2015. PMID: 26683323 Free PMC article.
-
Coronary Vasculature and Myocardial Structure in HIV: Physiologic Insights From the Renin-Angiotensin-Aldosterone System.J Clin Endocrinol Metab. 2021 Nov 19;106(12):3398-3412. doi: 10.1210/clinem/dgab112. J Clin Endocrinol Metab. 2021. PMID: 33624807 Free PMC article. Review.
References
-
- Ziegler-Heitbrock L, Ancuta P, Crowe S, Dalod M, Grau V, et al. (2010) Nomenclature of monocytes and dendritic cells in blood. Blood 116: e74–80. - PubMed
-
- Jalbert E, Crawford TQ, D'Antoni ML, Keating SM, Norris PJ, et al. (2013) IL-1Beta Enriched Monocytes Mount Massive IL-6 Responses to Common Inflammatory Triggers among Chronically HIV-1 Infected Adults on Stable Anti-Retroviral Therapy at Risk for Cardiovascular Disease. PLoS One 8: e75500. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
