

Physiological mechanisms of upper airway hypotonia during REM sleep
- PMID: 24587579
- PMCID: PMC3920322
- DOI: 10.5665/sleep.3498
Physiological mechanisms of upper airway hypotonia during REM sleep
Abstract
Study objectives: Rapid eye movement (REM)-induced hypotonia of the major upper airway dilating muscle (genioglossus) potentially contributes to the worsening of obstructive sleep apnea that occurs during this stage. No prior human single motor unit (SMU) study of genioglossus has examined this possibility to our knowledge. We hypothesized that genioglossus SMUs would reduce their activity during stable breathing in both tonic and phasic REM compared to stage N2 sleep. Further, we hypothesized that hypopneas occurring in REM would be associated with coincident reductions in genioglossus SMU activity.
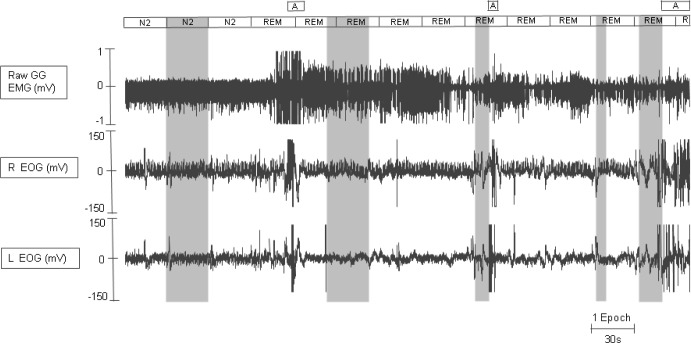
Design: The activity of genioglossus SMUs was studied in (1) neighboring epochs of stage N2, and tonic and phasic REM; and (2) during hypopneas occurring in REM.
Setting: Sleep laboratory.
Participants: 29 subjects (38 ± 13 y) (17 male).
Intervention: Natural sleep, including REM sleep and REM hypopneas.
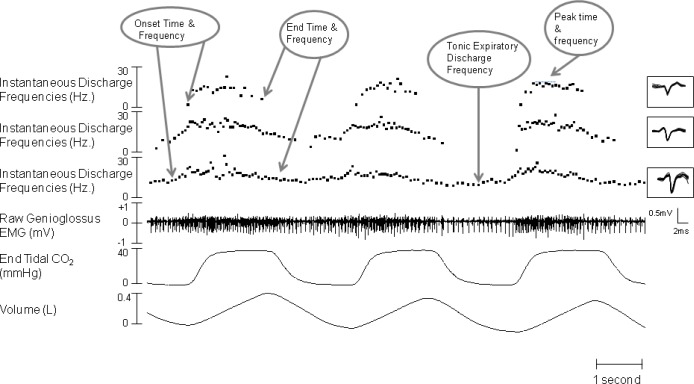
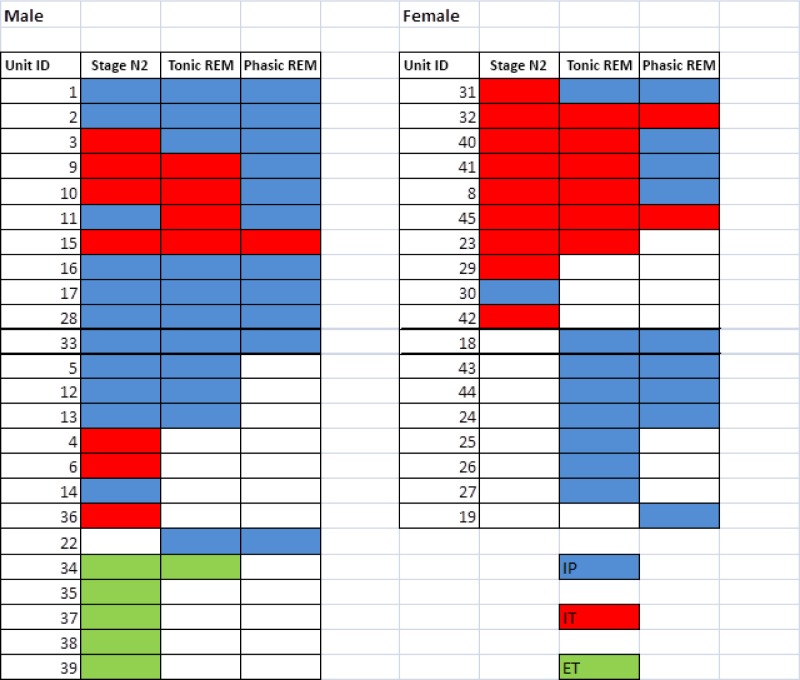
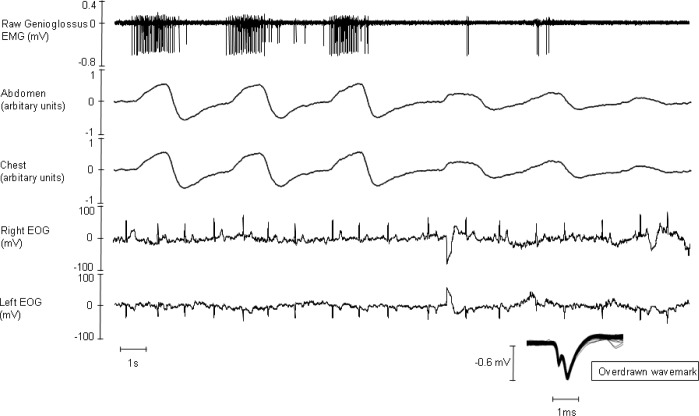
Measurement and results: Subjects slept overnight with genioglossus fine-wire intramuscular electrodes and full polysomnography. Forty-two SMUs firing during one or more of stage N2, tonic REM, or phasic REM were sorted. Twenty inspiratory phasic (IP), 17 inspiratory tonic (IT), and five expiratory tonic (ET) SMUs were characterized. Fewer units were active during phasic REM (23) compared to tonic REM (30) and stage N2 (33). During phasic REM sleep, genioglossus IP and IT SMUs discharged at slower rates and for shorter durations than during stage N2. For example, the SMU peak frequency during phasic REM 5.7 ± 6.6 Hz (mean ± standard deviation) was less than both tonic REM 12.3 ± 9.7 Hz and stage N2 16.1 ± 10.0 Hz (P < 0.001). The peak firing frequencies of IP/IT SMUs decreased from the last breath before to the first breath of a REM hypopnea (11.8 ± 10.9 Hz versus 5.7 ± 9.4 Hz; P = 0.001).
Conclusion: Genioglossus single motor unit activity is significantly reduced in REM sleep, particularly phasic REM. Single motor unit activity decreases abruptly at the onset of REM hypopneas.
Keywords: Obstructive sleep apnea; genioglossus; rapid eye movement sleep; single motor unit; upper airway hypotonia.
Figures
Similar articles
-
A mechanism for upper airway stability during slow wave sleep.Sleep. 2013 Apr 1;36(4):555-63. doi: 10.5665/sleep.2544. Sleep. 2013. PMID: 23565001 Free PMC article.
-
Neural drive to human genioglossus in obstructive sleep apnoea.J Physiol. 2007 Nov 15;585(Pt 1):135-46. doi: 10.1113/jphysiol.2007.139584. Epub 2007 Oct 4. J Physiol. 2007. PMID: 17916615 Free PMC article.
-
The influence of obstructive sleep apnea and gender on genioglossus activity during rapid eye movement sleep.Chest. 2009 Apr;135(4):957-964. doi: 10.1378/chest.08-2292. Epub 2008 Dec 31. Chest. 2009. PMID: 19118266 Free PMC article.
-
Airway dilator muscle activity and lung volume during stable breathing in obstructive sleep apnea.Sleep. 2009 Mar;32(3):361-8. doi: 10.1093/sleep/32.3.361. Sleep. 2009. PMID: 19294956 Free PMC article.
-
Discharge properties of upper airway motor units during wakefulness and sleep.Prog Brain Res. 2014;212:59-75. doi: 10.1016/B978-0-444-63488-7.00004-5. Prog Brain Res. 2014. PMID: 25194193 Review.
Cited by
-
Positive Airway Pressure Therapy for Pediatric Obstructive Sleep Apnea.Children (Basel). 2021 Oct 29;8(11):979. doi: 10.3390/children8110979. Children (Basel). 2021. PMID: 34828692 Free PMC article. Review.
-
Dynamic models of obstructive sleep apnea provide robust prediction of respiratory event timing and a statistical framework for phenotype exploration.Sleep. 2022 Dec 12;45(12):zsac189. doi: 10.1093/sleep/zsac189. Sleep. 2022. PMID: 35932480 Free PMC article.
-
Neural Control of the Upper Airway: Respiratory and State-Dependent Mechanisms.Compr Physiol. 2016 Sep 15;6(4):1801-1850. doi: 10.1002/cphy.c160002. Compr Physiol. 2016. PMID: 27783860 Free PMC article. Review.
-
Older adults at greater risk for Alzheimer's disease show stronger associations between sleep apnea severity and verbal memory.Res Sq [Preprint]. 2023 Dec 2:rs.3.rs-3683218. doi: 10.21203/rs.3.rs-3683218/v1. Res Sq. 2023. Update in: Alzheimers Res Ther. 2024 May 9;16(1):102. doi: 10.1186/s13195-024-01446-3. PMID: 38076899 Free PMC article. Updated. Preprint.
-
Sex differences in obstructive sleep apnea phenotypes, the multi-ethnic study of atherosclerosis.Sleep. 2020 May 12;43(5):zsz274. doi: 10.1093/sleep/zsz274. Sleep. 2020. PMID: 31687772 Free PMC article.
References
-
- Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328:1230–5. - PubMed
-
- Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365:1046–53. - PubMed
-
- McNicholas WT, Bonsigore MR. Sleep apnoea as an independent risk factor for cardiovascular disease: current evidence, basic mechanisms and research priorities. Eur Respir J. 2007;29:156–78. - PubMed
-
- Mulgrew AT, Nasvadi G, Butt A, et al. Risk and severity of motor vehicle crashes in patients with obstructive sleep apnoea/hypopnoea. Thorax. 2008;63:536–41. - PubMed
-
- Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med. 2005;353:2034–41. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
