

Percutaneous radiofrequency ablation for early hepatocellular carcinoma: risk factors for survival
- PMID: 24587635
- PMCID: PMC3925868
- DOI: 10.3748/wjg.v20.i6.1585
Percutaneous radiofrequency ablation for early hepatocellular carcinoma: risk factors for survival
Abstract
Aim: To evaluate outcomes of radiofrequency ablation (RFA) therapy for early hepatocellular carcinoma (HCC) and identify survival- and recurrence-related factors.
Methods: Consecutive patients diagnosed with early HCC by computed tomography (CT) or magnetic resonance imaging (MRI) (single nodule of ≤ 5 cm, or multi- (up to 3) nodules of ≤ 3 cm each) and who underwent RFA treatment with curative intent between January 2010 and August 2011 at the Instituto do Câncer do Estado de São Paulo, Brazil were enrolled in the study. RFA of the liver tumors (with 1.0 cm ablative margin) was carried out under CT-fluoro scan and ultrasonic image guidance of the percutaneous ablation probes. Procedure-related complications were recorded. At 1-mo post-RFA and 3-mo intervals thereafter, CT and MRI were performed to assess outcomes of complete response (absence of enhancing tissue at the tumor site) or incomplete response (enhancing tissue remaining at the tumor site). Overall survival and disease-free survival rates were estimated by the Kaplan-Meier method and compared by the log rank test or simple Cox regression. The effect of risk factors on survival was assessed by the Cox proportional hazard model.
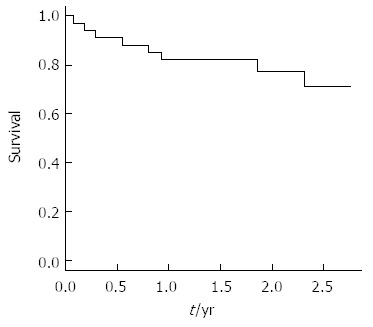
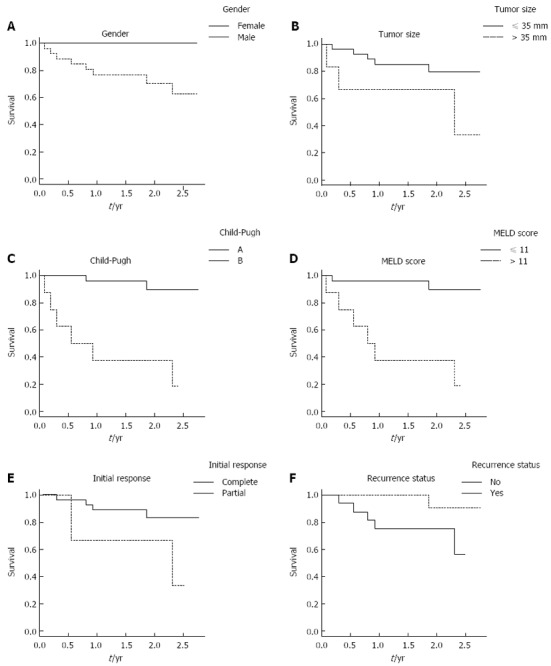
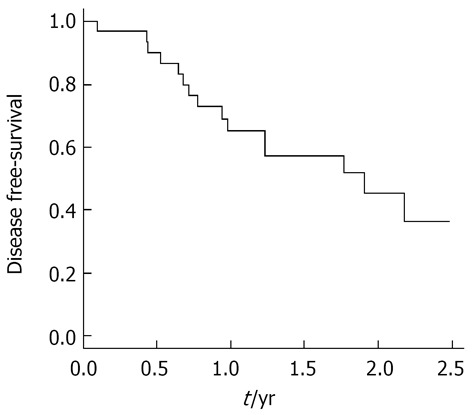
Results: A total of 38 RFA sessions were performed during the study period on 34 patients (age in years: mean, 63 and range, 49-84). The mean follow-up time was 22 mo (range, 1-33). The study population showed predominance of male sex (76%), less severe liver disease (Child-Pugh A, n = 26; Child-Pugh B, n = 8), and single tumor (65%). The maximum tumor diameters ranged from 10 to 50 mm (median, 26 mm). The initial (immediately post-procedure) rate of RFA-induced complete tumor necrosis was 90%. The probability of achieving complete response was significantly greater in patients with a single nodule (vs patients with multi-nodules, P = 0.04). Two patients experienced major complications, including acute pulmonary edema (resolved with intervention) and intestinal perforation (led to death). The 1- and 2-year overall survival rates were 82% and 71%, respectively. Sex, tumor size, initial response, and recurrence status influenced survival, but did not reach the threshold of statistical significance. Child-Pugh class and the model for end-stage liver disease score were identified as predictors of survival by simple Cox regression, but only Child-Pugh class showed a statistically significant association to survival in multiple Cox regression analysis (HR = 15; 95%CI: 3-76 mo; P = 0.001). The 1- and 2-year cumulative disease-free survival rates were 65% and 36%, respectively.
Conclusion: RFA is an effective therapy for local tumor control of early HCC, and patients with preserved liver function are the best candidates.
Keywords: Disease-free survival; Hepatocellular carcinoma; Overall survival; Radiofrequency ablation.
Figures
References
-
- Bosch FX, Ribes J, Díaz M, Cléries R. Primary liver cancer: worldwide incidence and trends. Gastroenterology. 2004;127:S5–S16. - PubMed
-
- Kikuchi L, Chagas AL, Alencar RS, Paranaguá-Vezozzo DC, Carrilho FJ. Clinical and epidemiological aspects of hepatocellular carcinoma in Brazil. Antivir Ther. 2013;18:445–449. - PubMed
-
- Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. Lancet. 2012;379:1245–1255. - PubMed
-
- Lencioni R. Loco-regional treatment of hepatocellular carcinoma. Hepatology. 2010;52:762–773. - PubMed
-
- Orlando A, Leandro G, Olivo M, Andriulli A, Cottone M. Radiofrequency thermal ablation vs. percutaneous ethanol injection for small hepatocellular carcinoma in cirrhosis: meta-analysis of randomized controlled trials. Am J Gastroenterol. 2009;104:514–524. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
