

Immunotherapy in gastric cancer
- PMID: 24587645
- PMCID: PMC3930966
- DOI: 10.3748/wjg.v20.i7.1657
Immunotherapy in gastric cancer
Abstract
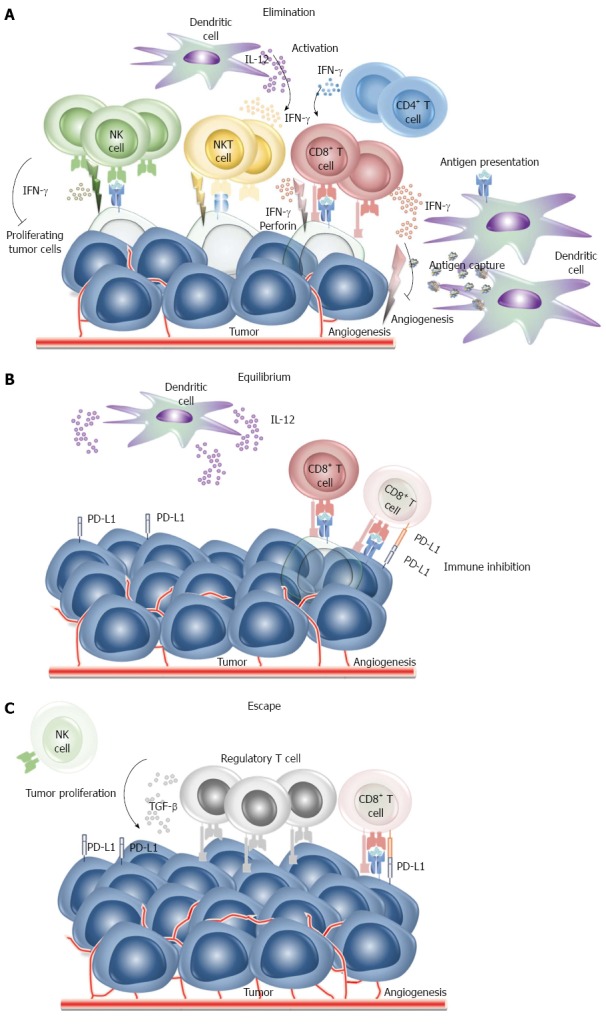
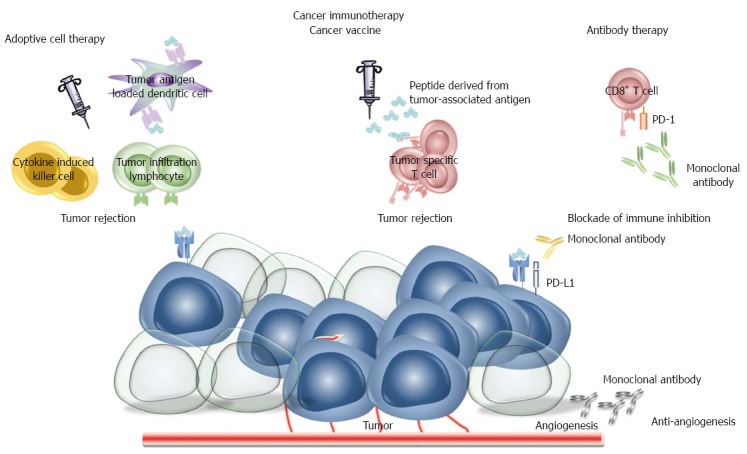
Gastric cancer is the second most common of cancer-related deaths worldwide. In the majority of cases gastric cancer is advanced at diagnosis and although medical and surgical treatments have improved, survival rates remain poor. Cancer immunotherapy has emerged as a powerful and promising clinical approach for treatment of cancer and has shown major success in breast cancer, prostate cancer and melanoma. Here, we provide an overview of concepts of modern cancer immunotherapy including the theory, current approaches, remaining hurdles to be overcome, and the future prospect of cancer immunotherapy in the treatment of gastric cancer. Adaptive cell therapies, cancer vaccines, gene therapies, monoclonal antibody therapies have all been used with some initial successes in gastric cancer. However, to date the results in gastric cancer have been disappointing as current approaches often do not stimulate immunity efficiently allowing tumors continue to grow despite the presence of a measurable immune response. Here, we discuss the identification of targets for immunotherapy and the role of biomarkers in prospectively identifying appropriate subjects or immunotherapy. We also discuss the molecular mechanisms by which tumor cells escape host immunosurveillance and produce an immunosuppressive tumor microenvironment. We show how advances have provided tools for overcoming the mechanisms of immunosuppression including the use of monoclonal antibodies to block negative regulators normally expressed on the surface of T cells which limit activation and proliferation of cytotoxic T cells. Immunotherapy has greatly improved and is becoming an important factor in such fields as medical care and welfare for human being. Progress has been rapid ensuring that the future of immunotherapy for gastric cancer is bright.
Keywords: Adoptive cell therapy; Antibody therapy; Cancer vaccine; Gastric cancer; Immune checkpoint; Immune escape; Predictive biomarker.
Figures
References
-
- Chiba T, Marusawa H, Ushijima T. Inflammation-associated cancer development in digestive organs: mechanisms and roles for genetic and epigenetic modulation. Gastroenterology. 2012;143:550–563. - PubMed
-
- Vollmers HP, Dämmrich J, Ribbert H, Wozniak E, Müller-Hermelink HK. Apoptosis of stomach carcinoma cells induced by a human monoclonal antibody. Cancer. 1995;76:550–558. - PubMed
-
- Rosenberg S. Lymphokine-activated killer cells: a new approach to immunotherapy of cancer. J Natl Cancer Inst. 1985;75:595–603. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
