

Perioperative anemia management in colorectal cancer patients: a pragmatic approach
- PMID: 24587673
- PMCID: PMC3934467
- DOI: 10.3748/wjg.v20.i8.1972
Perioperative anemia management in colorectal cancer patients: a pragmatic approach
Abstract
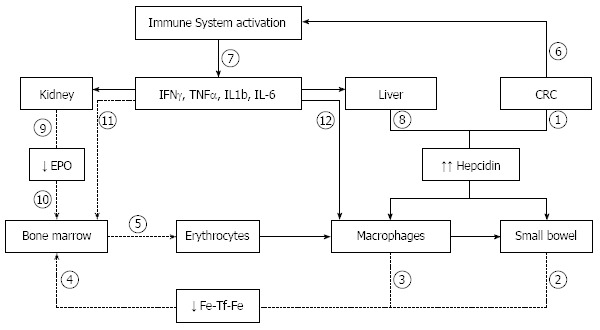
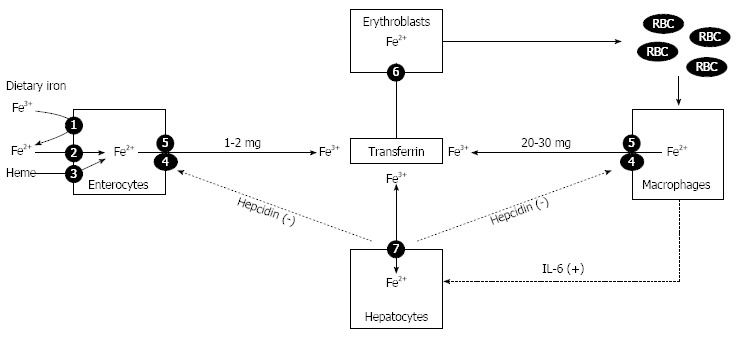
Anemia, usually due to iron deficiency, is highly prevalent among patients with colorectal cancer. Inflammatory cytokines lead to iron restricted erythropoiesis further decreasing iron availability and impairing iron utilization. Preoperative anemia predicts for decreased survival. Allogeneic blood transfusion is widely used to correct anemia and is associated with poorer surgical outcomes, increased post-operative nosocomial infections, longer hospital stays, increased rates of cancer recurrence and perioperative venous thromboembolism. Infections are more likely to occur in those with low preoperative serum ferritin level compared to those with normal levels. A multidisciplinary, multimodal, individualized strategy, collectively termed Patient Blood Management, minimizes or eliminates allogeneic blood transfusion. This includes restrictive transfusion policy, thromboprophylaxis and anemia management to improve outcomes. Normalization of preoperative hemoglobin levels is a World Health Organization recommendation. Iron repletion should be routinely ordered when indicated. Oral iron is poorly tolerated with low adherence based on published evidence. Intravenous iron is safe and effective but is frequently avoided due to misinformation and misinterpretation concerning the incidence and clinical nature of minor infusion reactions. Serious adverse events with intravenous iron are extremely rare. Newer formulations allow complete replacement dosing in 15-60 min markedly facilitating care. Erythropoiesis stimulating agents may improve response rates. A multidisciplinary, multimodal, individualized strategy, collectively termed Patient Blood Management used to minimize or eliminate allogeneic blood transfusion is indicated to improve outcomes.
Keywords: Allogeneic blood transfusion; Anemia; Colorectal cancer; Erythropoiesis stimulating agents; Intravenous iron; Patient Blood Management.
Figures
References
-
- Cappell MS, Goldberg ES. The relationship between the clinical presentation and spread of colon cancer in 315 consecutive patients. A significant trend of earlier cancer detection from 1982 through 1988 at a university hospital. J Clin Gastroenterol. 1992;14:227–235. - PubMed
-
- Sadahiro S, Suzuki T, Tokunaga N, Mukai M, Tajima T, Makuuchi H, Saito T. Anemia in patients with colorectal cancer. J Gastroenterol. 1998;33:488–494. - PubMed
-
- Ludwig H, Van Belle S, Barrett-Lee P, Birgegård G, Bokemeyer C, Gascón P, Kosmidis P, Krzakowski M, Nortier J, Olmi P, et al. The European Cancer Anaemia Survey (ECAS): a large, multinational, prospective survey defining the prevalence, incidence, and treatment of anaemia in cancer patients. Eur J Cancer. 2004;40:2293–2306. - PubMed
-
- Beale AL, Penney MD, Allison MC. The prevalence of iron deficiency among patients presenting with colorectal cancer. Colorectal Dis. 2005;7:398–402. - PubMed
-
- Prutki M, Poljak-Blazi M, Jakopovic M, Tomas D, Stipancic I, Zarkovic N. Altered iron metabolism, transferrin receptor 1 and ferritin in patients with colon cancer. Cancer Lett. 2006;238:188–196. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
