

The recognition and evaluation of patterns of compensatory injury in patients with mechanical hip pain
- PMID: 24587859
- PMCID: PMC3931342
- DOI: 10.1177/1941738114522201
The recognition and evaluation of patterns of compensatory injury in patients with mechanical hip pain
Abstract
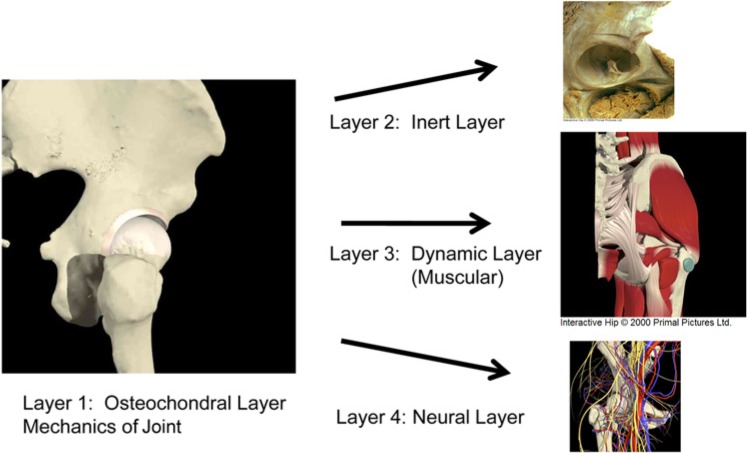
Context: In active individuals with femoroacetabular impingement (FAI), the resultant reduction in functional range of motion leads to high impaction loads at terminal ranges. These increased forces result in compensatory effects on bony and soft tissue structures within the hip joint and hemipelvis. An algorithm is useful in evaluating athletes with pre-arthritic, mechanical hip pain and associated compensatory disorders.
Evidence acquisition: A literature search was performed by a review of PubMed articles published from 1976 to 2013.
Level of evidence: Level 4.
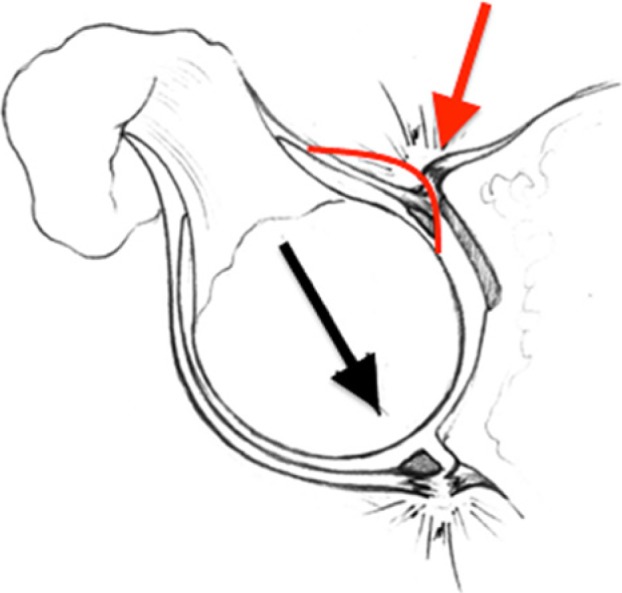
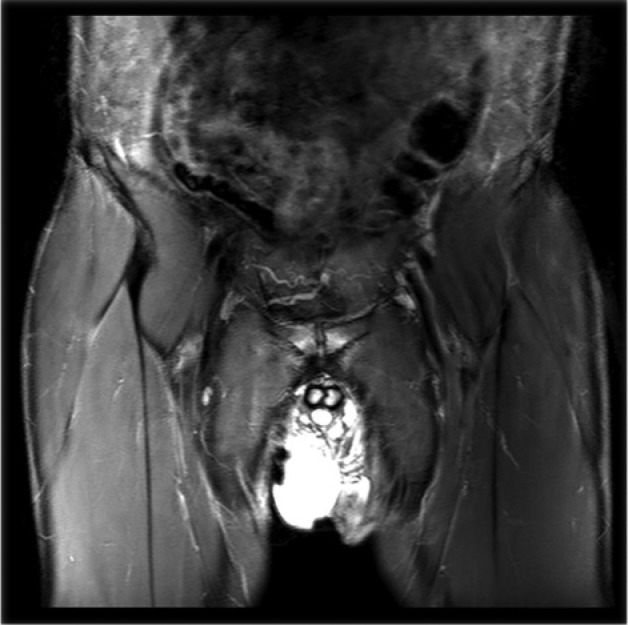
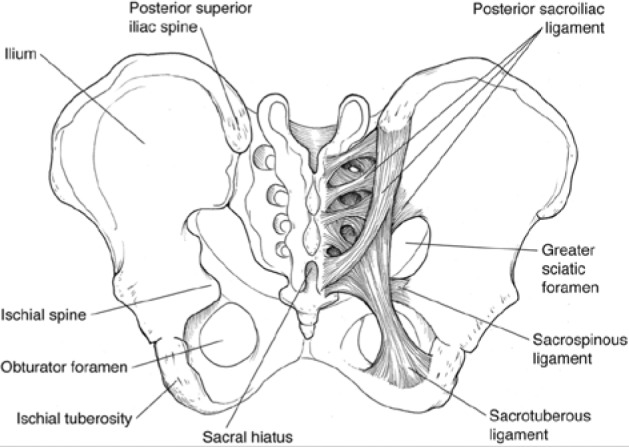
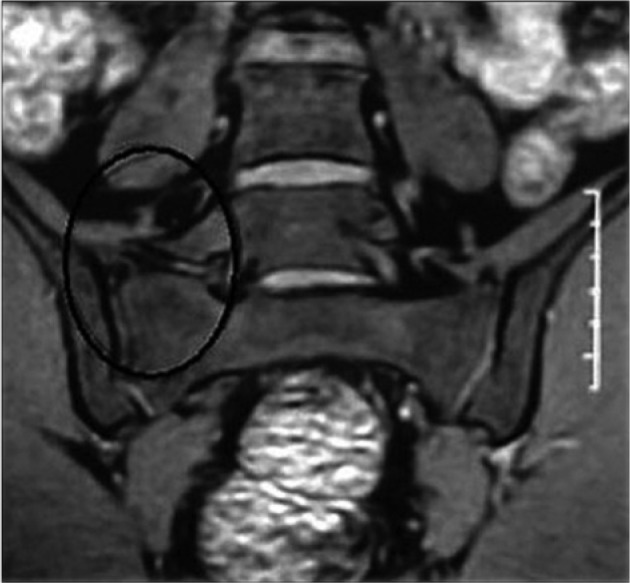
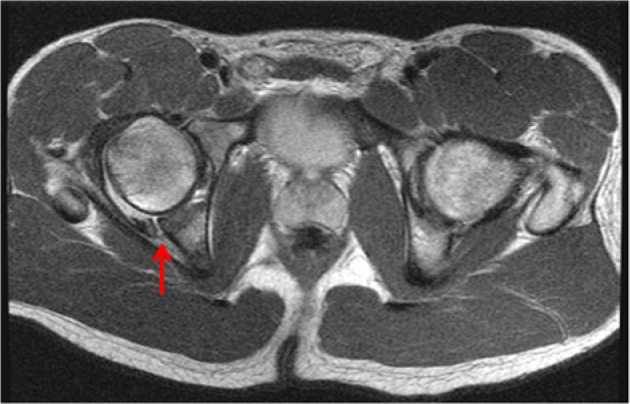
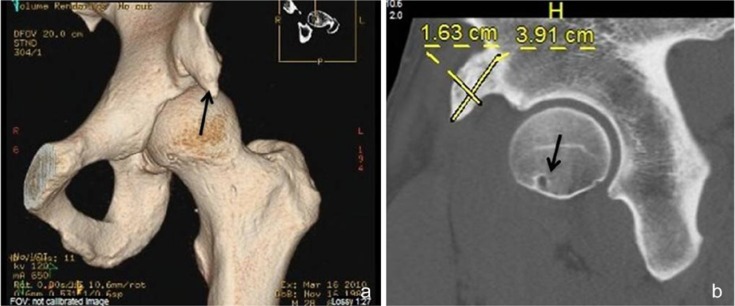
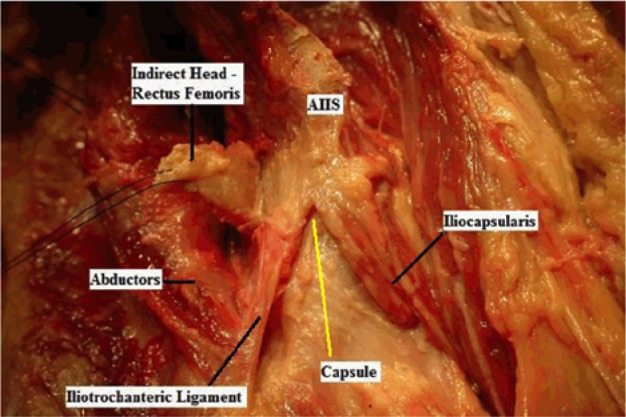
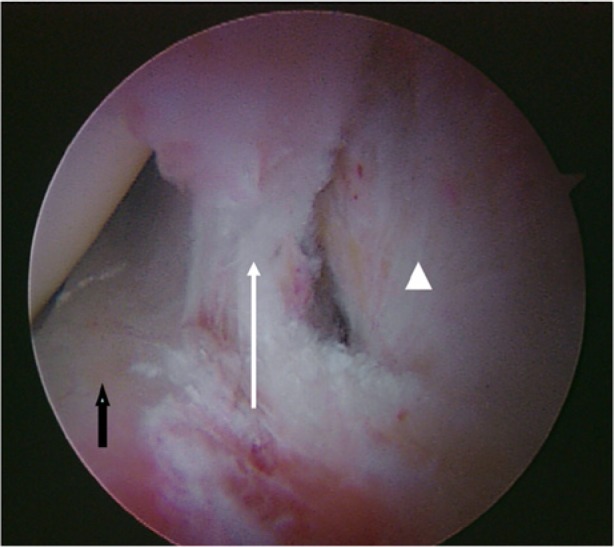
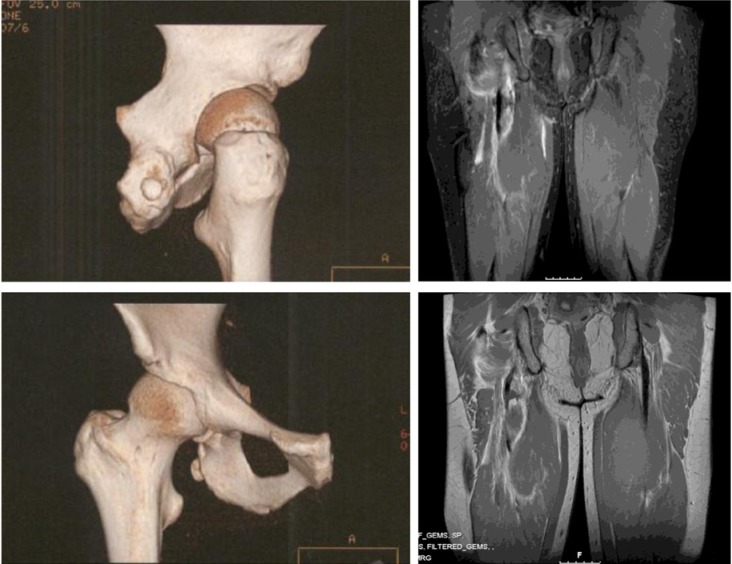
Results: Increased stresses across the bony hemipelvis result when athletes with FAI attempt to achieve supraphysiologic, terminal ranges of motion (ROM) through the hip joint required for athletic competition. This can manifest as pain within the pubic joint (osteitis pubis), sacroiliac joint, and lumbosacral spine. Subclinical posterior hip instability may result when attempts to increase hip flexion and internal rotation are not compensated for by increased motion through the hemipelvis. Prominence of the anterior inferior iliac spine (AIIS) at the level of the acetabular rim can result in impingement of the anterior hip joint capsule or iliocapsularis muscle origin against the femoral head-neck junction, resulting in a distinct form of mechanical hip impingement (AIIS subspine impingement). Iliopsoas impingement (IPI) has also been described as an etiology for anterior hip pain. IPI results in a typical 3-o'clock labral tear as well as an inflamed capsule in close proximity to the overlying iliopsoas tendon. Injury in athletic pubalgia occurs during high-energy twisting activities in which abnormal hip ROM and resultant pelvic motion lead to shearing across the pubic symphysis.
Conclusion: Failure to recognize and address concomitant compensatory injury patterns associated with intra-articular hip pathology can result in significant disability and persistent symptoms in athletes with pre-arthritic, mechanical hip pain.
Strength-of-recommendation taxonomy sort: B.
Keywords: athletic pubalgia; compensatory injury; femoroacetabular impingement; hip; iliopsoas impingement.
Conflict of interest statement
The following authors declared potential conflicts of interest: Asheesh Bedi, MD, is an education consultant for Smith & Nephew.
Figures


Similar articles
-
Anatomic footprint of the direct head of the rectus femoris origin: cadaveric study and clinical series of hips after arthroscopic anterior inferior iliac spine/subspine decompression.Arthroscopy. 2013 Dec;29(12):1932-40. doi: 10.1016/j.arthro.2013.08.023. Epub 2013 Oct 18. Arthroscopy. 2013. PMID: 24140143
-
Femoroacetabular Impingement Patients With Decreased Femoral Version Have Different Impingement Locations and Intra- and Extraarticular Anterior Subspine FAI on 3D-CT-Based Impingement Simulation: Implications for Hip Arthroscopy.Am J Sports Med. 2019 Nov;47(13):3120-3132. doi: 10.1177/0363546519873666. Epub 2019 Sep 20. Am J Sports Med. 2019. PMID: 31539275
-
Arthroscopic Decompression of the Anterior Inferior Iliac Spine.JBJS Essent Surg Tech. 2023 May 11;13(2):e22.00019. doi: 10.2106/JBJS.ST.22.00019. eCollection 2023 Apr-Jun. JBJS Essent Surg Tech. 2023. PMID: 38274146 Free PMC article.
-
Non-femoroacetabular impingement.Semin Musculoskelet Radiol. 2013 Jul;17(3):279-85. doi: 10.1055/s-0033-1348094. Epub 2013 Jun 20. Semin Musculoskelet Radiol. 2013. PMID: 23787982 Review.
-
Current concepts in the diagnosis and management of extra-articular hip impingement syndromes.Int Orthop. 2017 Jul;41(7):1321-1328. doi: 10.1007/s00264-017-3431-4. Epub 2017 Apr 11. Int Orthop. 2017. PMID: 28401279 Review.
Cited by
-
Posterior hip instability relocation testing: a resident's case report.J Man Manip Ther. 2017 Sep;25(4):215-220. doi: 10.1080/10669817.2017.1318522. Epub 2017 May 2. J Man Manip Ther. 2017. PMID: 28912634 Free PMC article.
-
Rectus femoris ossification accompanying with sacroiliac joint edema.Turk J Phys Med Rehabil. 2021 Mar 4;67(1):125-126. doi: 10.5606/tftrd.2021.5145. eCollection 2021 Mar. Turk J Phys Med Rehabil. 2021. PMID: 33948556 Free PMC article. No abstract available.
-
The prevalence and risk factors of pubic bone marrow edema in femoroacetabular impingement and hip dysplasia.J Hip Preserv Surg. 2021 Nov 9;8(4):318-324. doi: 10.1093/jhps/hnab081. eCollection 2021 Dec. J Hip Preserv Surg. 2021. PMID: 35505801 Free PMC article.
-
Open MRI assessment of anterior femoroacetabular clearance in active and passive impingement-provoking postures.Bone Jt Open. 2021 Nov;2(11):988-996. doi: 10.1302/2633-1462.211.BJO-2021-0143. Bone Jt Open. 2021. PMID: 34825828 Free PMC article.
-
Arthroscopic Capsular Reconstruction of the Hip With Acellular Dermal Extracellular Matrix: Surgical Technique.Arthrosc Tech. 2016 Sep 5;5(5):e1001-e1005. doi: 10.1016/j.eats.2016.05.002. eCollection 2016 Oct. Arthrosc Tech. 2016. PMID: 27909667 Free PMC article.
References
-
- Ahumada LA, Ashruf S, Espinosa-de-los-Monteros A, et al. Athletic pubalgia: definition and surgical treatment. Ann Plast Surg. 2005;55:393-396 - PubMed
-
- Anderson K, Strickland SM, Warren R. Hip and groin injuries in athletes. Am J Sports Med. 2001;29:521-533 - PubMed
-
- Anderson SA, Keene JS. Results of arthroscopic iliopsoas tendon release in competitive and recreational athletes. Am J Sports Med. 2008;36:2363-2371 - PubMed
-
- Antolak SJ, Jr, Hough DM, Pawlina W, Spinner RJ. Anatomical basis of chronic pelvic pain syndrome: the ischial spine and pudendal nerve entrapment. Med Hypotheses. 2002;59:349-353 - PubMed
-
- Armfield DR, Kim DH, Towers JD, Bradley JP, Robertson DD. Sports-related muscle injury in the lower extremity. Clin Sports Med. 2006;25:803-842 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
