

Is Repeat PTA of a Failing Hemodialysis Fistula Durable?
- PMID: 24587906
- PMCID: PMC3920629
- DOI: 10.1155/2014/369687
Is Repeat PTA of a Failing Hemodialysis Fistula Durable?
Abstract
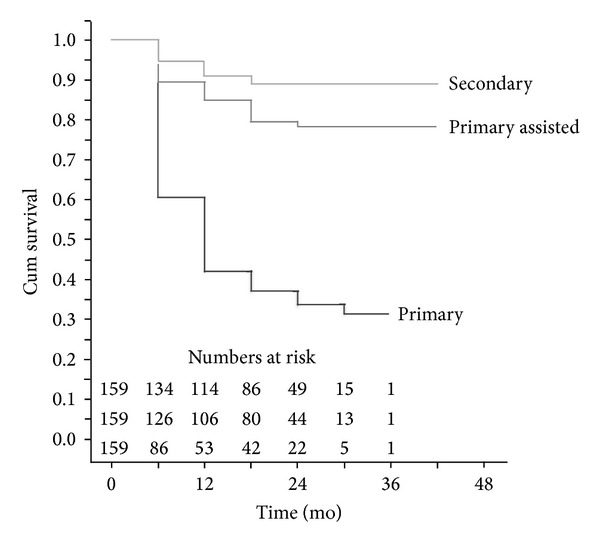
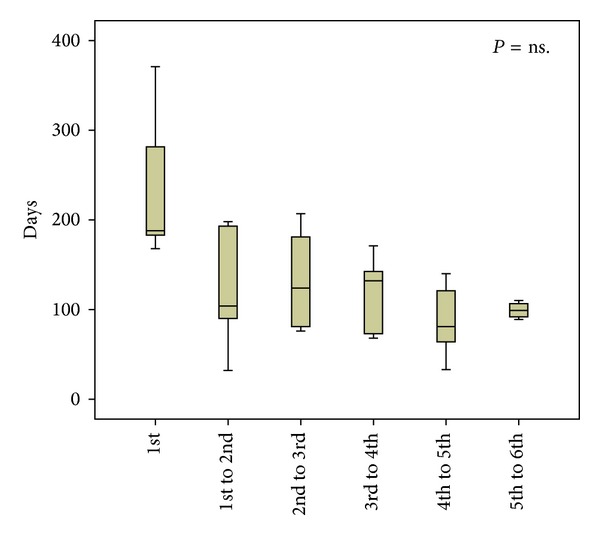
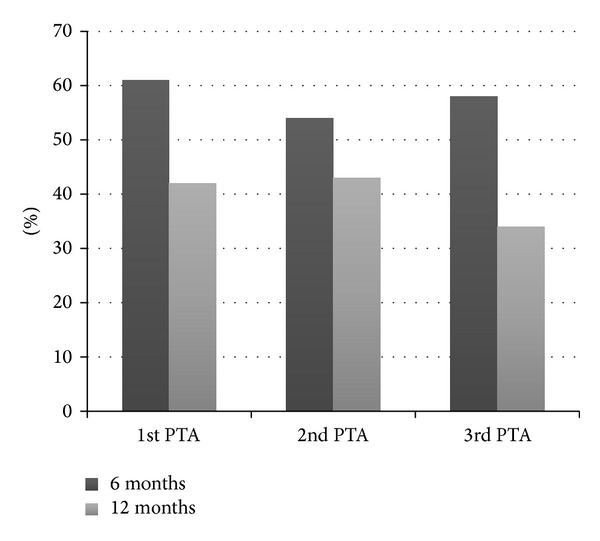
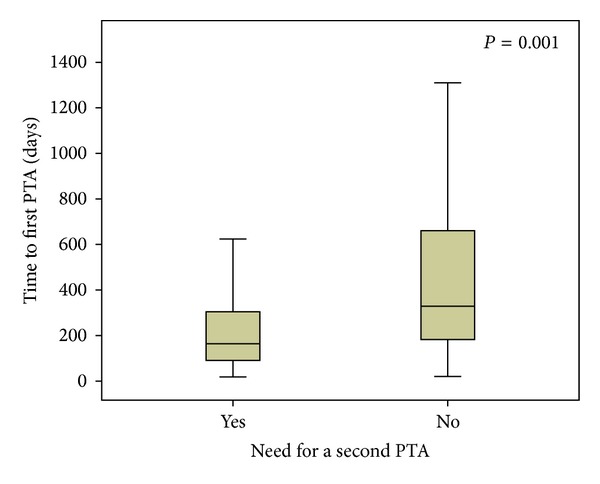
Purpose. Our objective was to evaluate the outcome of percutaneous transluminal angioplasty (PTA) and particularly rePTA in a failing arteriovenous fistula (AV-fistula). Are multiple redilations worthwhile? Patients and Methods. All 159 stenoses of AV fistulas that were treated with PTA, with or without stenting, during 2008 and 2009, were included. Occluded fistulas that were dilated after successful thrombolysis were also included. Median age was 68 (interquartile range 61.5-78.5) years and 75% were male. Results. Seventy-nine (50%) of the primary PTAs required no further reintervention. The primary patency was 61% at 6 months and 42% at 12 months. Eighty (50%) of the stenoses needed at least one reintervention. Primary assisted patency (defined as patency after subsequent reinterventions) was 89% at 6 months and 85% at 12 months. The durability of repeated PTAs was similar to the durability of the primary PTA. However, an early primary PTA carried a higher risk for subsequent reinterventions. Successful dialysis was achieved after 98% of treatments. Nine percent of the stenoses eventually required surgical revision and 13% of the fistulas failed permanently. Conclusion. The present study suggests that most failing AV-fistulas can be salvaged endovascularly. Repeated PTA seems similarly durable as the primary PTA.
Figures
References
-
- Svenskt Njurregister (SNR) Aktiv uremivård i Sverige1991–2009. http://www.medscinet.net/snr/rapporter.aspx.
-
- Dapunt O, Feurstein M, Rendl KH, Prenner K. Transluminal angioplasty versus conventional operation in the treatment of haemodialysis fistula stenosis: results from a 5-year study. British Journal of Surgery. 1987;74(11):1004–1005. - PubMed
-
- Hingorani A, Ascher E, Kallakuri S, Greenberg S, Khanimov Y. Impact of reintervention for failing upper-extremity arteriovenous autogenous access for hemodialysis. Journal of Vascular Surgery. 2001;34(6):1004–1009. - PubMed
-
- Tessitore N, Mansueto G, Lipari G, et al. Endovascular versus surgical preemptive repair of forearm arteriovenous fistula juxta-anastomotic stenosis: analysis of data collected prospectively from 1999 to 2004. Clinical Journal of the American Society of Nephrology. 2006;1(3):448–454. - PubMed
-
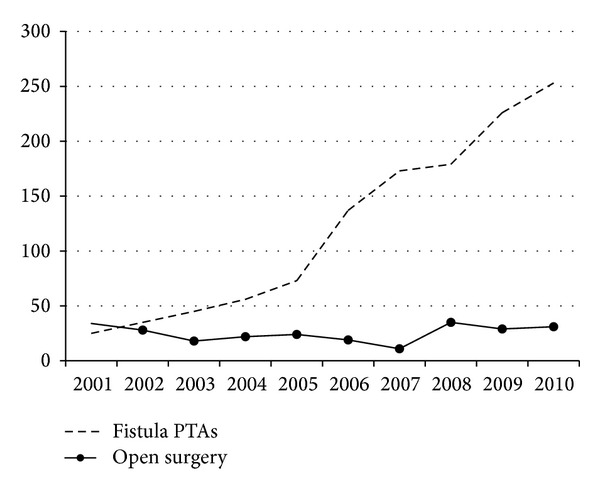
- Ljungström KG, Troeng T, Björck M. Time-trends in vascular access surgery in Sweden. European Journal of Vascular & Endovascular Surgery. 2008;36(5):592–596. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
