

Stem Cells and Healing: Impact on Inflammation
- PMID: 24587974
- PMCID: PMC3842880
- DOI: 10.1089/wound.2013.0449
Stem Cells and Healing: Impact on Inflammation
Abstract
Significance: The number of patients with nonhealing wounds has rapidly accelerated over the past 10 years in both the United States and worldwide. Some causative factors at the macro level include an aging population, epidemic numbers of obese and diabetic patients, and an increasing number of surgical procedures. At the micro level, chronic inflammation is a consistent finding.
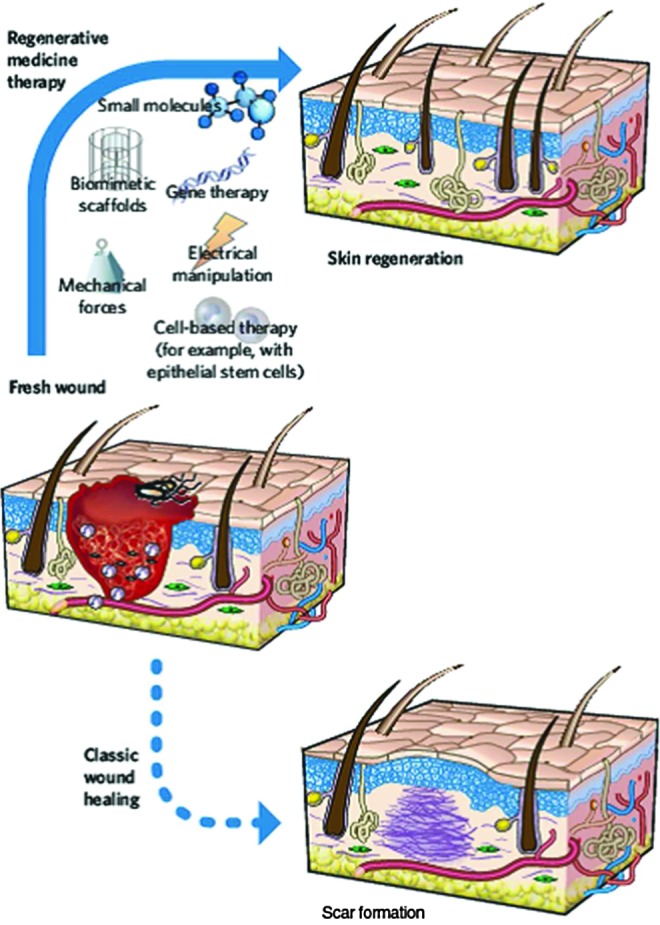
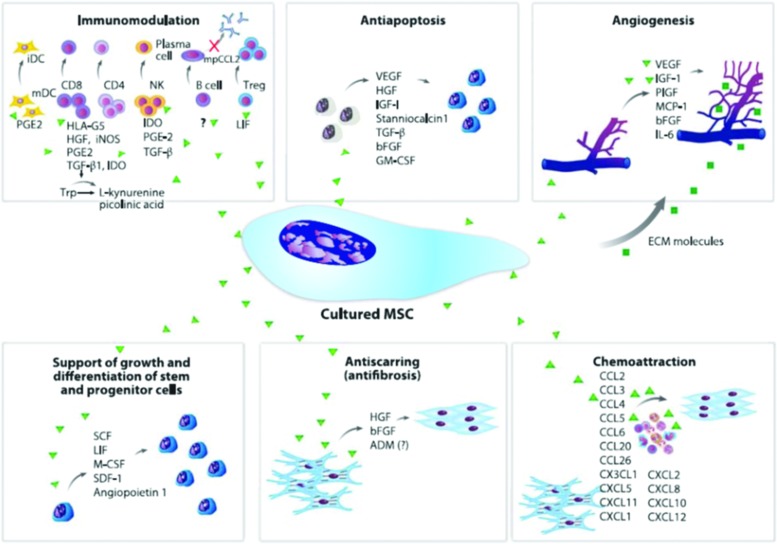
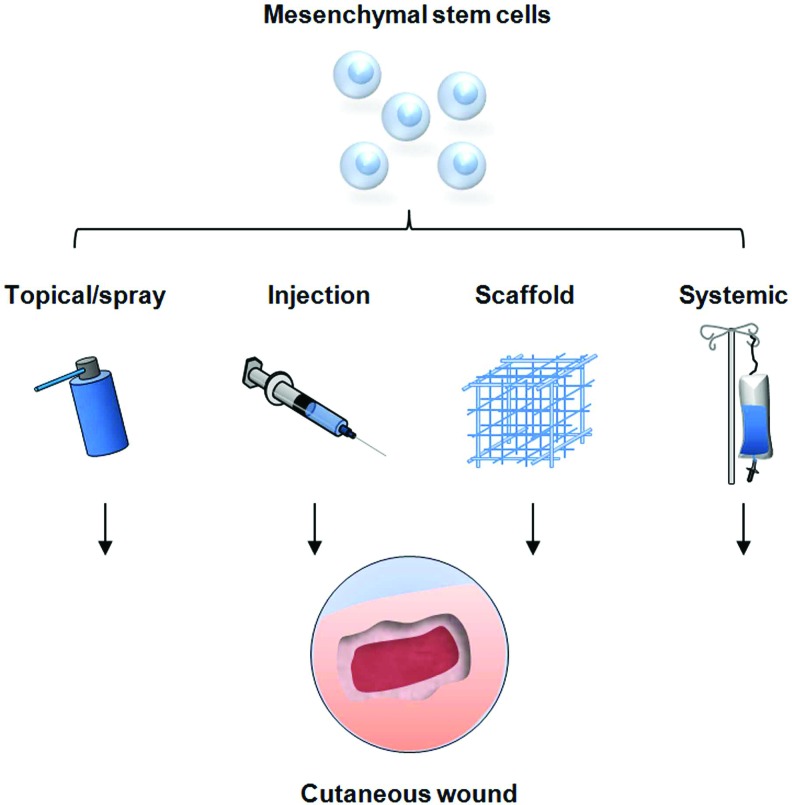
Recent advances: A number of treatment modalities are currently used to accelerate wound healing, including energy-based modalities, scaffoldings, the use of mechano-transduction, cytokines/growth factors, and cell-based therapies. The use of stem cell therapy has been hypothesized as a potentially useful adjunct for nonhealing wounds. Specifically, mesenchymal stem cells (MSCs) have been shown to improve wound healing in several studies. Immune modulating properties of MSCs have made them attractive treatment options.
Critical issues: Current limitations of stem cell therapy include the potentially large number of cells required for an effect, complex preparation and delivery methods, and poor cell retention in targeted tissues. Comparisons of published in-vitro and clinical trials are difficult due to cell preparation techniques, passage number, and the impact of the micro-environment on cell behavior.
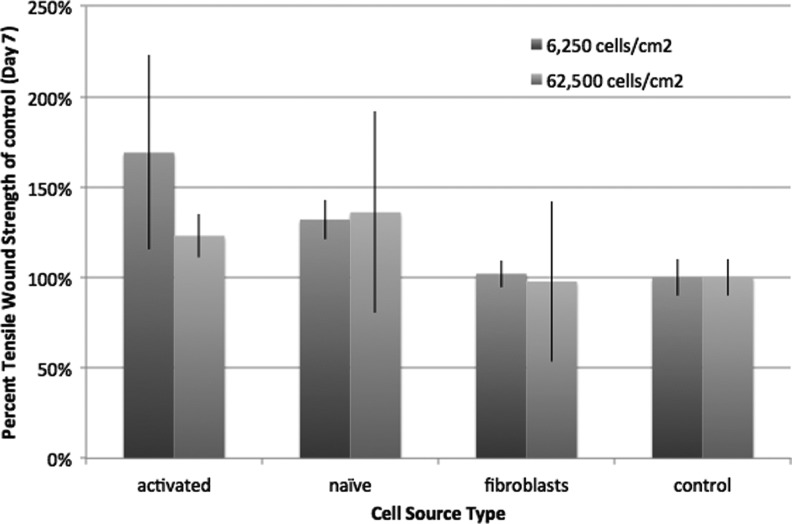
Future directions: MSCs may be more useful if they are preactivated with inflammatory cytokines such as tumor necrosis factor alpha or interferon gamma. This article will review the current literature with regard to the use of stem cells for wound healing. In addition the anti-inflammatory effects of MSCs will be discussed along with the potential benefits of stem cell preactivation.
Figures

Similar articles
-
Mesenchymal Stem Cells in Chronic Wounds: The Spectrum from Basic to Advanced Therapy.Adv Wound Care (New Rochelle). 2016 Apr 1;5(4):149-163. doi: 10.1089/wound.2015.0627. Adv Wound Care (New Rochelle). 2016. PMID: 27076993 Free PMC article. Review.
-
Mesenchymal Stem Cells for Chronic Wound Healing: Current Status of Preclinical and Clinical Studies.Tissue Eng Part B Rev. 2020 Dec;26(6):555-570. doi: 10.1089/ten.TEB.2019.0351. Epub 2020 May 20. Tissue Eng Part B Rev. 2020. PMID: 32242479 Review.
-
Mesenchymal stem cells-derived MFG-E8 accelerates diabetic cutaneous wound healing.J Dermatol Sci. 2017 Jun;86(3):187-197. doi: 10.1016/j.jdermsci.2017.02.285. Epub 2017 Mar 6. J Dermatol Sci. 2017. PMID: 28302404
-
Mesenchymal Stem Cell Therapy for Cutaneous Wounds.Adv Wound Care (New Rochelle). 2012 Aug;1(4):166-171. doi: 10.1089/wound.2011.0294. Adv Wound Care (New Rochelle). 2012. PMID: 24527299 Free PMC article. Review.
-
The Role of Mesenchymal Stem Cells in the Regenerative Wound Healing Phenotype.Adv Wound Care (New Rochelle). 2012 Aug;1(4):159-165. doi: 10.1089/wound.2012.0361. Adv Wound Care (New Rochelle). 2012. PMID: 24527298 Free PMC article. Review.
Cited by
-
Deciphering the crosstalk between inflammation and biofilm in chronic wound healing: Phytocompounds loaded bionanomaterials as therapeutics.Saudi J Biol Sci. 2024 Apr;31(4):103963. doi: 10.1016/j.sjbs.2024.103963. Epub 2024 Feb 23. Saudi J Biol Sci. 2024. PMID: 38425782 Free PMC article. Review.
-
Challenges in the Treatment of Chronic Wounds.Adv Wound Care (New Rochelle). 2015 Sep 1;4(9):560-582. doi: 10.1089/wound.2015.0635. Adv Wound Care (New Rochelle). 2015. PMID: 26339534 Free PMC article. Review.
-
A Rheological Study on the Effect of Tethering Pro- and Anti-Inflammatory Cytokines into Hydrogels on Human Mesenchymal Stem Cell Migration, Degradation, and Morphology.Biomacromolecules. 2024 Aug 12;25(8):5121-5137. doi: 10.1021/acs.biomac.4c00508. Epub 2024 Jul 3. Biomacromolecules. 2024. PMID: 38961715 Free PMC article.
-
Wound healing complications in oncological patients: perspectives for cellular therapy.Postepy Dermatol Alergol. 2019 Apr;36(2):139-146. doi: 10.5114/ada.2018.72585. Epub 2018 Jan 4. Postepy Dermatol Alergol. 2019. PMID: 31320845 Free PMC article. Review.
-
Mechanoresponse of stem cells for vascular repair.World J Stem Cells. 2019 Dec 26;11(12):1104-1114. doi: 10.4252/wjsc.v11.i12.1104. World J Stem Cells. 2019. PMID: 31875871 Free PMC article. Review.
References
-
- Mirza R. Koh TJ. Dysregulation of monocyte/macrophage phenotype in wounds of diabetic mice. Cytokine. 2011;56:256. - PubMed
-
- Gurtner GC. Werner S. Barrandon Y. Longaker MT. Wound repair and regeneration. Nature. 2008;453:314. - PubMed
-
- Limova M. Active wound coverings: bioengineered skin and dermal substitutes. Surg Clin North Am. 2010;90:1237. - PubMed
-
- Rheinwald JG. Green H. Serial cultivation of strains of human epidermal keratinocytes: the formation of keratinizing colonies from single cells. Cell. 1975;6:331. - PubMed
-
- Falanga V. Sabolinski M. A bilayered living skin construct (APLIGRAF) accelerates complete closure of hard-to-heal venous ulcers. Wound Repair Regen. 1999;7:201. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
