

An arranged marriage for precision medicine: hypoxia and genomic assays in localized prostate cancer radiotherapy
- PMID: 24588670
- PMCID: PMC4064607
- DOI: 10.1259/bjr.20130753
An arranged marriage for precision medicine: hypoxia and genomic assays in localized prostate cancer radiotherapy
Abstract
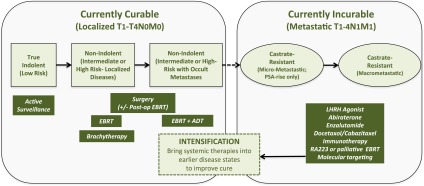
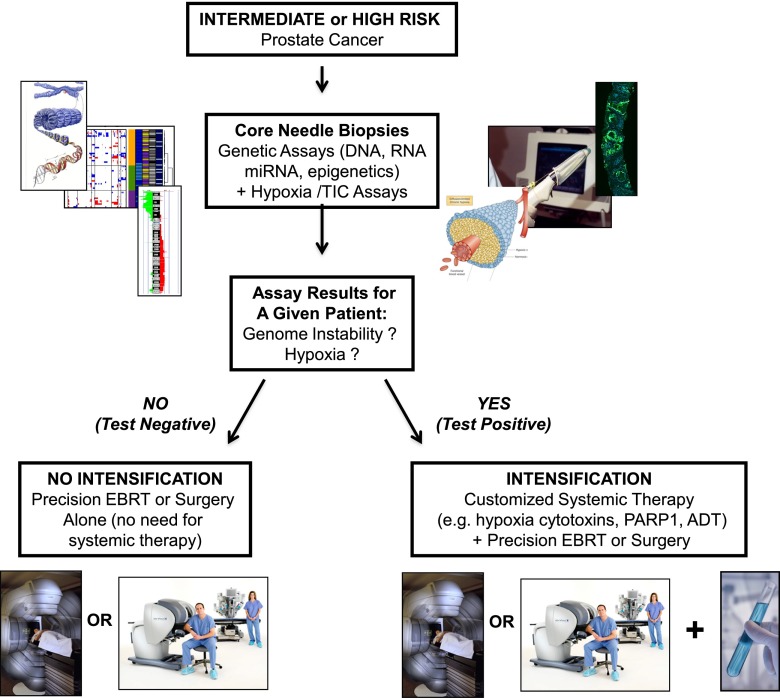
Prostate cancer (CaP) is the most commonly diagnosed malignancy in males in the Western world with one in six males diagnosed in their lifetime. Current clinical prognostication groupings use pathologic Gleason score, pre-treatment prostatic-specific antigen and Union for International Cancer Control-TNM staging to place patients with localized CaP into low-, intermediate- and high-risk categories. These categories represent an increasing risk of biochemical failure and CaP-specific mortality rates, they also reflect the need for increasing treatment intensity and justification for increased side effects. In this article, we point out that 30-50% of patients will still fail image-guided radiotherapy or surgery despite the judicious use of clinical risk categories owing to interpatient heterogeneity in treatment response. To improve treatment individualization, better predictors of prognosis and radiotherapy treatment response are needed to triage patients to bespoke and intensified CaP treatment protocols. These should include the use of pre-treatment genomic tests based on DNA or RNA indices and/or assays that reflect cancer metabolism, such as hypoxia assays, to define patient-specific CaP progression and aggression. More importantly, it is argued that these novel prognostic assays could be even more useful if combined together to drive forward precision cancer medicine for localized CaP.
Figures
Comment in
-
Pre-radiotherapy identification of individual genomic profile to avoid, by resort to customized radiosensitizers, the risk of radioresistance development in patients with localized prostate cancer.Br J Radiol. 2015 Jan;88(1045):20140630. doi: 10.1259/bjr.20140630. Br J Radiol. 2015. PMID: 25363844 Free PMC article. No abstract available.
-
Pre-radiotherapy identification of individual genomic profile to avoid, by resort to customized radiosensitizers, the risk of radioresistance development in patients with localized prostate cancer: author reply.Br J Radiol. 2015 Jan;88(1045):20140701. doi: 10.1259/bjr.20140701. Br J Radiol. 2015. PMID: 25363875 Free PMC article. No abstract available.
References
-
- D'Amico AV, Moul J, Carroll PR, Sun L, Lubeck D, Chen MH. Cancer-specific mortality after surgery or radiation for patients with clinically localized prostate cancer managed during the prostate-specific antigen era. J Clin Oncol 2003; 21: 2163–72. - PubMed
-
- Grimm P, Billiet I, Bostwick D, Dicker AP, Frank S, Immerzeel J, et al. Comparative analysis of prostate-specific antigen free survival outcomes for patients with low, intermediate and high risk prostate cancer treatment by radical therapy. Results from the Prostate Cancer Results Study Group. BJU Int 2012; 110: E431–2. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
