

Pegloticase immunogenicity: the relationship between efficacy and antibody development in patients treated for refractory chronic gout
- PMID: 24588936
- PMCID: PMC4060440
- DOI: 10.1186/ar4497
Pegloticase immunogenicity: the relationship between efficacy and antibody development in patients treated for refractory chronic gout
Abstract
Introduction: The efficacy of pegloticase, a polyethylene glycol (PEG)-conjugated mammalian recombinant uricase, approved for chronic refractory gout, can be limited by the development of antibodies (Ab). Analyses from 2 replicate, 6-month, randomized controlled trials were performed to characterize Ab responses to pegloticase.
Methods: Anti-pegloticase, anti-PEG, and anti-uricase Ab were determined by validated enzyme-linked immunosorbent assays. Ab titers were analyzed for possible relationships with serum pegloticase concentrations, serum uric acid (sUA) lowering, and risk of infusion reactions (IRs).
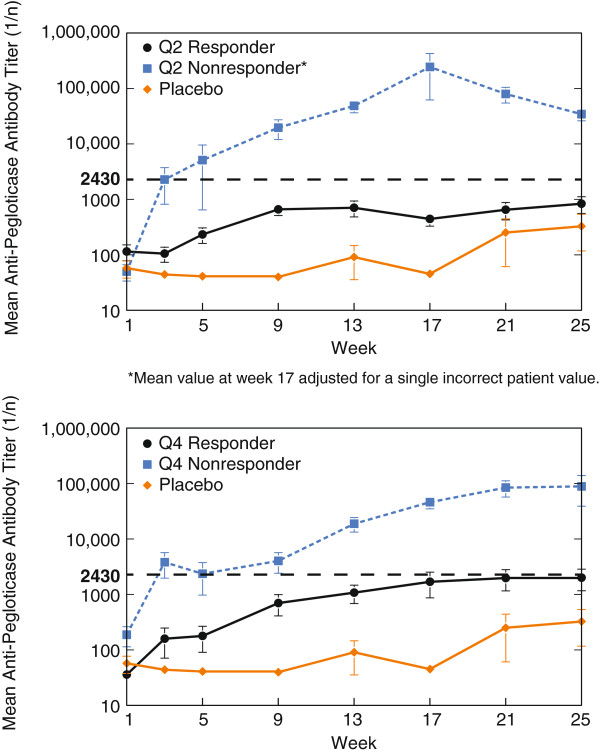
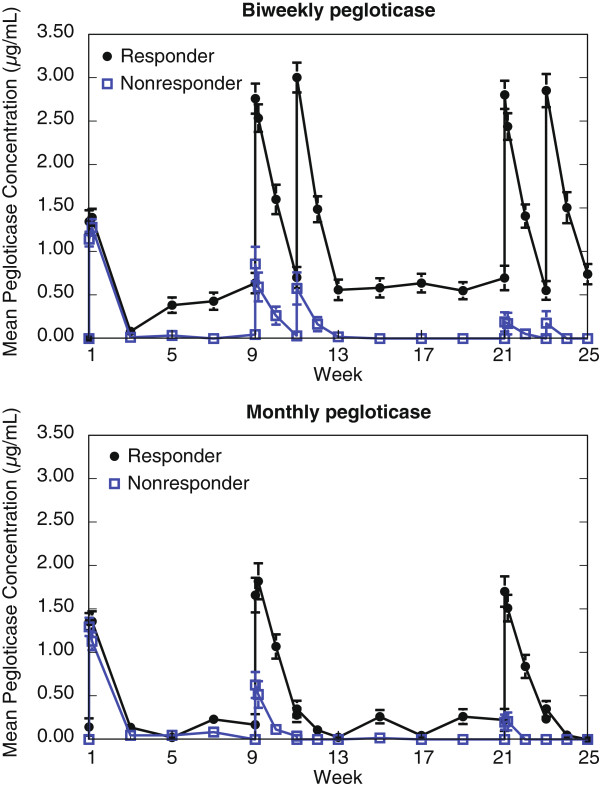
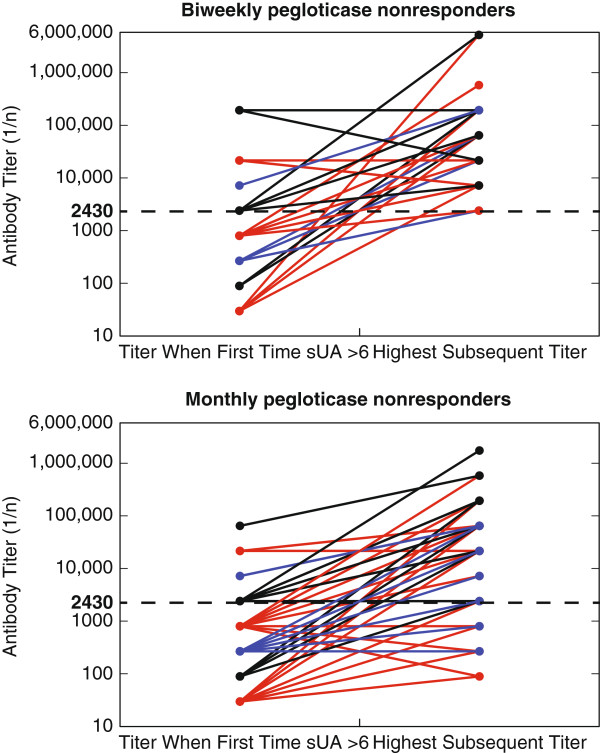
Results: Sixty-nine (41%) of 169 patients receiving pegloticase developed high titer anti-pegloticase Ab (> 1:2430) and 40% (67/169) developed anti-PEG Ab; 1 patient receiving placebo developed high titer anti-pegloticase Ab. Only 14% (24/169) of patients developed anti-uricase Ab, usually at low titer. In responders, patients showing sustained UA lowering, mean anti-pegloticase titers at week 25 (1:837 ± 1687 with biweekly and 1:2025 ± 4506 with monthly dosing) were markedly lower than in nonresponders (1:34,528 ± 42,228 and 1:89,658 ± 297,797, respectively). Nonresponder status was associated with reduced serum pegloticase concentrations. Baseline anti-pegloticase Ab, evident in 15% (31/212) of patients, did not predict subsequent loss of urate-lowering response. Loss of sUA response preceded IRs in 44 of 56 (79%) pegloticase-treated patients.
Conclusions: Loss of responsiveness to pegloticase is associated with the development of high titer anti-pegloticase Ab that increase clearance of pegloticase and are associated with a loss of the sUA lowering effect and increased IR risk. Pre-infusion sUA can be used as a surrogate for the presence of deleterious anti-pegloticase Ab.
Trial registration: NCT00325195. Registered 10 May 2006, NCT01356498. Registered 27 October 2008.
Figures

Comment in
-
PEG-ing down (and preventing?) the cause of pegloticase failure.Arthritis Res Ther. 2014 May 30;16(3):112. doi: 10.1186/ar4572. Arthritis Res Ther. 2014. PMID: 25142440 Free PMC article.
References
-
- Mandell BF. Clinical manifestations of hyperuricemia and gout. Cleve Clin J Med. 2008;75:S5–S8. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
