

Impact of compliance with infection management guidelines on outcome in patients with severe sepsis: a prospective observational multi-center study
- PMID: 24589043
- PMCID: PMC4057316
- DOI: 10.1186/cc13755
Impact of compliance with infection management guidelines on outcome in patients with severe sepsis: a prospective observational multi-center study
Abstract
Introduction: Current sepsis guidelines recommend antimicrobial treatment (AT) within one hour after onset of sepsis-related organ dysfunction (OD) and surgical source control within 12 hours. The objective of this study was to explore the association between initial infection management according to sepsis treatment recommendations and patient outcome.
Methods: In a prospective observational multi-center cohort study in 44 German ICUs, we studied 1,011 patients with severe sepsis or septic shock regarding times to AT, source control, and adequacy of AT. Primary outcome was 28-day mortality.
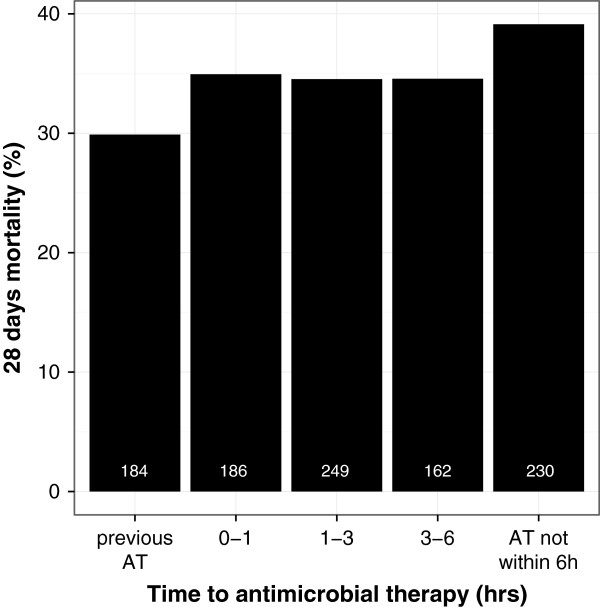
Results: Median time to AT was 2.1 (IQR 0.8 - 6.0) hours and 3 hours (-0.1 - 13.7) to surgical source control. Only 370 (36.6%) patients received AT within one hour after OD in compliance with recommendation. Among 422 patients receiving surgical or interventional source control, those who received source control later than 6 hours after onset of OD had a significantly higher 28-day mortality than patients with earlier source control (42.9% versus 26.7%, P <0.001). Time to AT was significantly longer in ICU and hospital non-survivors; no linear relationship was found between time to AT and 28-day mortality. Regardless of timing, 28-day mortality rate was lower in patients with adequate than non-adequate AT (30.3% versus 40.9%, P < 0.001).
Conclusions: A delay in source control beyond 6 hours may have a major impact on patient mortality. Adequate AT is associated with improved patient outcome but compliance with guideline recommendation requires improvement. There was only indirect evidence about the impact of timing of AT on sepsis mortality.
Figures
Comment in
-
It's not just the antibiotics, it's the treatment.Crit Care. 2014 Jun 3;18(3):147. doi: 10.1186/cc13904. Crit Care. 2014. PMID: 25043513 Free PMC article.
References
-
- Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, Sevransky JE, Sprung CL, Douglas IS, Jaeschke R, Osborn TM, Nunnally ME, Townsend SR, Reinhart K, Kleinpell RM, Angus DC, Deutschman CS, Machado FR, Rubenfeld GD, Webb SA, Beale RJ, Vincent JL, Moreno R. Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41:580–637. doi: 10.1097/CCM.0b013e31827e83af. - DOI - PubMed
-
- Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, Sharma S, Suppes R, Feinstein D, Zanotti S, Taiberg L, Gurka D, Cheang M. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006;34:1589–1596. doi: 10.1097/01.CCM.0000217961.75225.E9. - DOI - PubMed
-
- Levy MM, Dellinger RP, Townsend SR, Linde-Zwirble WT, Marshall JC, Bion J, Schorr C, Artigas A, Ramsay G, Beale R, Parker MM, Gerlach H, Reinhart K, Silva E, Harvey M, Regan S, Angus DC. The surviving sepsis campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Crit Care Med. 2010;38:367–374. doi: 10.1097/CCM.0b013e3181cb0cdc. - DOI - PubMed
-
- Gaieski DF, Mikkelsen ME, Band RA, Pines JM, Massone R, Furia FF, Shofer FS, Goyal M. Impact of time to antibiotics on survival in patients with severe sepsis or septic shock in whom early goal-directed therapy was initiated in the emergency department. Crit Care Med. 2010;38:1045–1053. doi: 10.1097/CCM.0b013e3181cc4824. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
