

Review
doi: 10.1183/09059180.00007413.
Allergic aspergillosis of the respiratory tract
Affiliations
- PMID: 24591658
- PMCID: PMC9487274
- DOI: 10.1183/09059180.00007413
Item in Clipboard
Review
Allergic aspergillosis of the respiratory tract
Eur Respir Rev.
.
No abstract available
Conflict of interest statement
Statement of Interest: None declared.
Figures

Chest radiograph showing a non-homogeneous opacity in the right mid zone with perihilar patchy infiltrates in the left mid and lower zones. Transient pulmonary infiltrates or fleeting shadows that are characteristic of allergic bronchopulmonary asperillosis are visible.

Chest radiograph of the same patient as in figure 1 taken 18 months later showing a large consolidation in the right upper and mid zones with partial resolution of the left-sided perihilar infiltrate. In addition, blunting of the right costophrenic angle suggestive of pleural effusion can be seen. Transient pulmonary infiltrates or fleeting shadows that are characteristic of allergic bronchopulmonary asperillosis are visible.

Chest radiograph showing characteristic wine glass opacity in the left upper zone. A non-homogeneous consolidation is also seen on the right side.
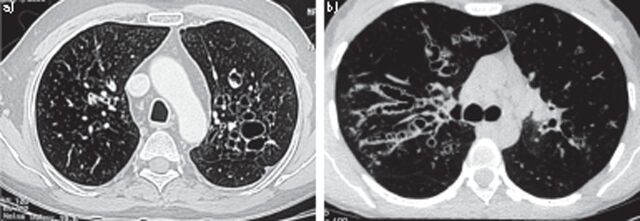
a) Computed tomography of the thorax showing signet ring appearances, indicative of central bronchiectasis. Mucoid impaction and dilated bronchi are also visible. b) Computed tomography of the thorax showing string of pearls appearances bilaterally, indicative of central bronchiectasis.
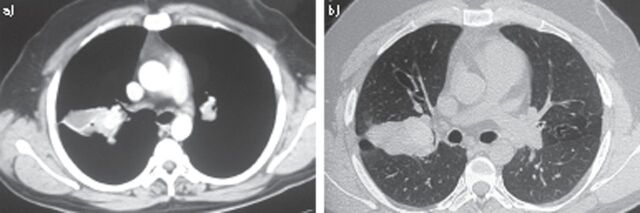
High-resolution computed tomography of the thorax a) mediastinal window and b) corresponding section on the lung window showing high attenuation mucus impaction.

Computed tomography of the paranasal sinuses showing hyperdense lesions in the frontal, ethmoid and maxillary sinuses bilaterally, suggestive of inspissated secretions.
References
-
- Shah A. Allergic bronchopulmonary aspergillosis. Indian J Chest Dis Allied Sci 1998; 40: 41–54. - PubMed
-
- de Shazo RD, Chapin K, Swain RE. Fungal sinusitis. N Engl J Med 1997; 337: 254–259. - PubMed
-
- Shah A, Panjabi C. Allergic bronchopulmonary aspergillosis: a review of a disease with a worldwide distribution. J Asthma 2002; 39: 273–289. - PubMed
-
- Longbottom JL, Pepys J. Pulmonary aspergillosis, diagnostic and immunological significance of antigens and C-reactive substance in Aspergillus fumigatus. J Pathol Bacteriol 1964; 88: 141–151. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical