

Comparison of the ultrashort gonadotropin-releasing hormone agonist-antagonist protocol with microdose flare -up protocol in poor responders: a preliminary study
- PMID: 24591934
- PMCID: PMC3939149
- DOI: 10.5152/jtgga.2010.35
Comparison of the ultrashort gonadotropin-releasing hormone agonist-antagonist protocol with microdose flare -up protocol in poor responders: a preliminary study
Abstract
Objective: To determine the potential effect of the ultrashort gonadotropin-releasing hormone (GnRH) agonist/GnRH antagonist protocol versus the microdose GnRH agonist protocol in poor responders undergoing intracytoplasmic sperm injection (ICSI).
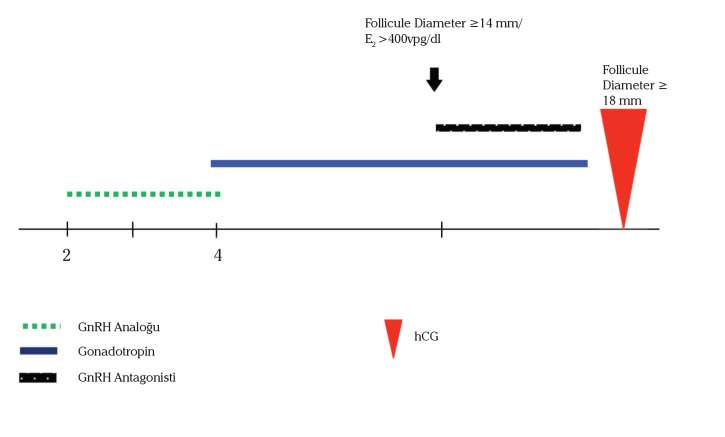
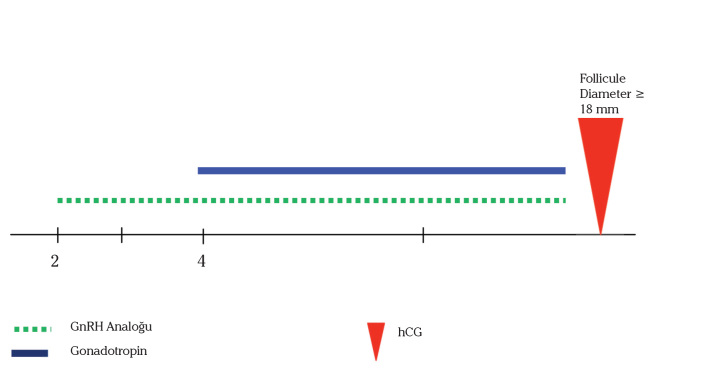
Material and methods: The patients in the Agonist-Antagonist Group (n=41) were administered the ultrashort GnRH-agonist/ antagonist protocol, while the patients in the Microdose Group (n=41) were stimulated according to the microdose flare-up protocol. The mean number of mature oocytes retrieved was the primary outcome measure. Fertilization rate, implantation rate per embryo and clinical pregnancy rates were secondary outcome measures.
Results: There was no differenc between the mean number of mature oocytes retrieved in the two groups. There were also no statistical differences between the two groups in terms of peak serum E2 level, canceled cycles, endometrial thickness on hCG day, number of 2 pronucleus and number of embryos transferred. However, the total gonadotropin consumption and duration of stimulation were significantly higher with the Agonist-Antagonist Group compared with the Microdose Group. The implantation and clinical pregnancy rates were similar between the two groups.
Conclusion: Despite the high dose of gonadotropin consumption and longer duration of stimulation with the ultrashort GnRH agonist/ antagonist protocol, it seems that the Agonist-Antagonist Protocol is not inferior to the microdose protocol in poor responders undergoing ICSI.
Amaç: ICSI uygulanan zayıf over cevaplı hastalarda ultra kısa GnRH agonist/GnRH antagonist protokolünün mikrodoz GnRH agonist protokolüne karşı potansiyel etkisini belirlemek.
Gereç ve yöntemler: Mikrodoz grubundaki (n=41) hastalar mikrodoz flare up protokolüne uygun olarak stimüle edilirken Agonist-Antagonist grubundaki (n=41) hastalara da ultra kısa GnRH-agonist/antagonist protokolü uygulandı. Bu çalışmanın primer sonuç değeri toplanan ortalama matür oosit sayısı iken, fertilizasyon oranı, embryo başına implantasyon oranı ve klinik gebelik oranı da sekonder sonuç değerleriydi.
Bulgular: İki grup arasındaki toplanan ortalama matür oosit sayıları arasında fark yoktu. Serum E2 düzeyleri, iptal edilen sikluslar, hCG günü endometrial kalınlığı, 2 pronukleus sayıları ve transfer edilen embryo sayılarında da iki grup arasında istatistiksel farklılıklar yoktu. Bununla birlikte Agonist-Antagonist grubunda total gonadotropin tüketimi ve stimülasyon süresi Mikrodoz grubuyla karşılaştırıldığında belirgin olarak daha yüksekti. İki grup arasındaki implantasyon ve klinik gebelik oranları ise birbirine benzerdi.
Sonuç: Ultra kısa GnRH agonist/ antagonist protokolü ile yüksek doz gonadotropin tüketimi ve daha uzun süreli stimülasyona rağmen ICSI uygulanan zayıf over cevaplı hastalarda Agonist-Antagonist Protokolünün mikrodoz protokolünden daha az etkili olmadığı görülmektedir.
Keywords: Agonist-Antagonist protocol; Poor responder; mature oocytes; microdose flare-up protocol.
Figures
References
-
- Jenkins JM, Davies DW, Devonport H, Anthony FW, Gadd SC, Watson RH, et al. Comparison of “poor” responders with “good” responders using a standard buserelin/human menopausal gonadotrophin regime for in-vitro fertilization. Hum Reprod. 1991;6:918–21. - PubMed
-
- Pellicer A, Lightman A, Diamond MP, Russell JB, DeCherney AH. Outcome of in vitro fertilization in women with low response to ovarian stimulation. Fertil Steril. 1987;47:812–5. - PubMed
-
- Keay SD, Liversedge NH, Mathur RS, Jenkins JM. Assisted conception following poor ovarian response to gonadotrophin stimulation. Br J Obstet Gynaecol. 1997;104:521–7. - PubMed
-
- Schoolcraft WB, Surrey ES, Minjarez DA, Stevens JM, Gardner DK. Management of poor responders: can outcomes be improved with a novel gonadotropin-releasing hormone antagonist/letrozole protocol? Fertil Steril. 2008;89:151–6. - PubMed
-
- Surrey ES, Schoolcraft WB. Evaluating strategies for improving ovarian response of the poor responder undergoing assisted reproductive techniques. Fertil Steril. 2000;73:667–76. - PubMed
LinkOut - more resources
Full Text Sources