

Phenotyping community-acquired pneumonia according to the presence of acute respiratory failure and severe sepsis
- PMID: 24593040
- PMCID: PMC4015148
- DOI: 10.1186/1465-9921-15-27
Phenotyping community-acquired pneumonia according to the presence of acute respiratory failure and severe sepsis
Abstract
Background: Acute respiratory failure (ARF) and severe sepsis (SS) are possible complications in patients with community-acquired pneumonia (CAP). The aim of the study was to evaluate prevalence, characteristics, risk factors and impact on mortality of hospitalized patients with CAP according to the presence of ARF and SS on admission.
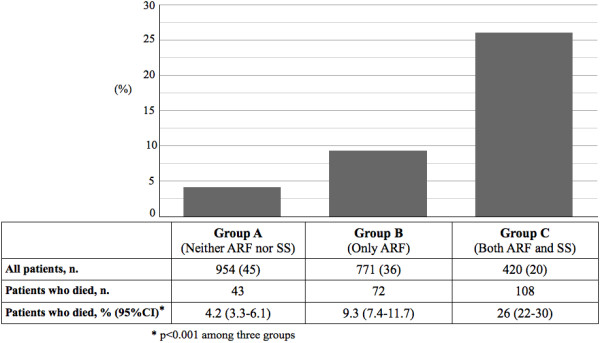
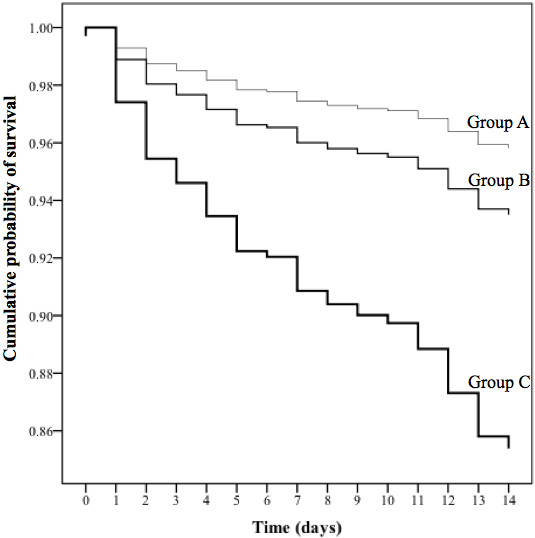
Methods: This was a multicenter, observational, prospective study of consecutive CAP patients admitted to three hospitals in Italy, Spain, and Scotland between 2008 and 2010. Three groups of patients were identified: those with neither ARF nor SS (Group A), those with only ARF (Group B) and those with both ARF and SS (Group C) on admission.
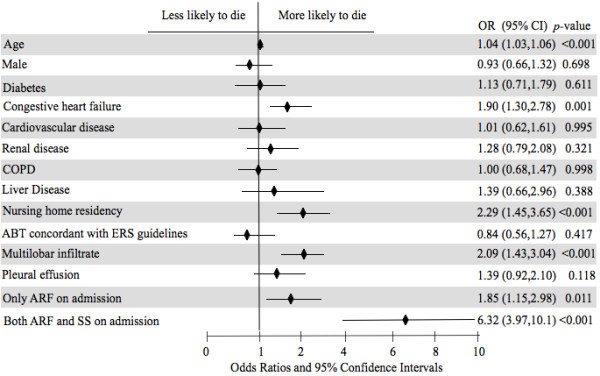
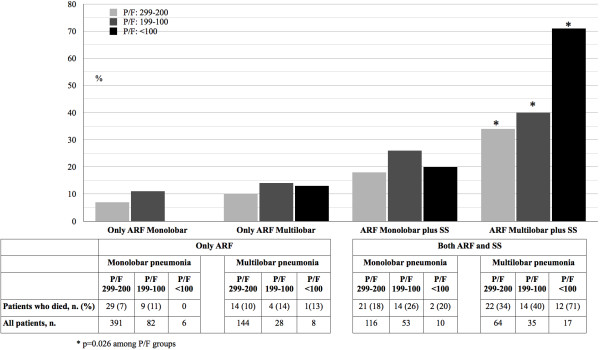
Results: Among the 2,145 patients enrolled, 45% belonged to Group A, 36% to Group B and 20% to Group C. Patients in Group C were more severe than patients in Group B. Isolated ARF was correlated with age (p < 0.001), COPD (p < 0.001) and multilobar infiltrates (p < 0.001). The contemporary occurrence of ARF and SS was associated with age (p = 0.002), residency in nursing home (p = 0.007), COPD (p < 0.001), multilobar involvement (p < 0.001) and renal disease (p < 0.001). 4.2% of patients in Group A died, 9.3% in Group B and 26% in Group C, p < 0.001. After adjustment, the presence of only ARF had an OR for in-hospital mortality of 1.85 (p = 0.011) and the presence of both ARF and SS had an OR of 6.32 (p < 0.001).
Conclusions: The identification of ARF and SS on hospital admission can help physicians in classifying CAP patients into three different clinical phenotypes.
Figures
References
-
- Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, Dowell SF, File TM jr, Musher DM, Niederman MS, Torres A, Whitney CG. Infectious diseases society of America/American thoracic society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44 Suppl 2:S27–S72. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
