

Sigmoid colocolic fistula caused by intrauterine device migration: a case report
- PMID: 24594141
- PMCID: PMC3946035
- DOI: 10.1186/1752-1947-8-81
Sigmoid colocolic fistula caused by intrauterine device migration: a case report
Abstract
Introduction: The intrauterine device is a form of contraception with a long duration of action and few systemic side effects. Migration into the abdominal cavity may occur early or years after insertion giving rise to bowel obstruction, perforation, ischemia, mesenteric injury, strictures or fistulae. Colocolic fistula formation is a rare but serious complication of intrauterine device migration, which may lead to difficulties in diagnosis and device retrieval.
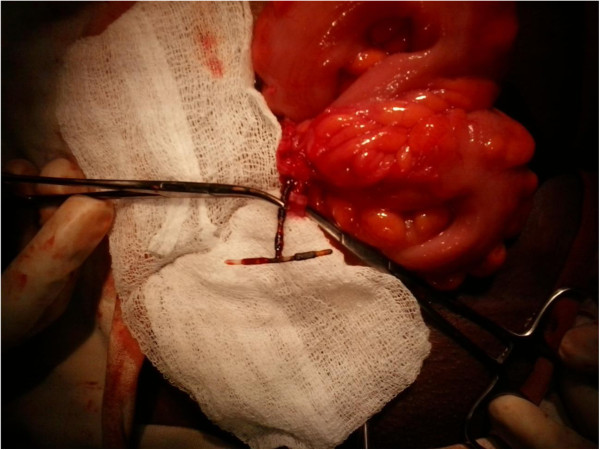
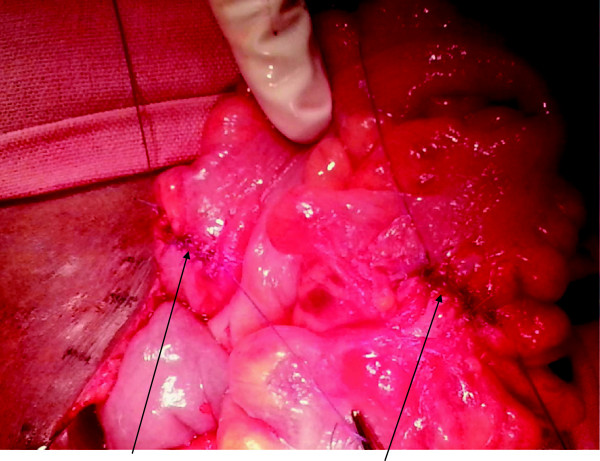
Case presentation: We report the case of a 29-year-old Sri Lankan woman who became pregnant 5 years after intrauterine device insertion. The device could not be located during pregnancy. She was asymptomatic and defaulted follow up during the antenatal period. She had an uncomplicated vaginal delivery. A subsequent laparotomy for device retrieval failed due to technical difficulties. A repeat laparotomy identified a sigmoid colocolic fistula with adhesions to the fallopian tube. The device was removed and colonic defects primarily closed following which the patient made an uneventful recovery.
Conclusions: All translocated intrauterine devices should be removed regardless of type and location. This case illustrates that they may cause complex bowel lesions leading to serious technical difficulties during retrieval. With the increasing use of minimally invasive approaches for intrauterine device retrieval, a low threshold for open surgery in complicated cases is advocated.
Figures

References
-
- Prabhu JK, Rani R, Nayak NK, Natarajan P. Migration of intrauterine contraceptive device into sigmoid colon. J ObstetGynaecol. 2010;30:526–527. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
