

Th1 response and systemic treg deficiency in inclusion body myositis
- PMID: 24594700
- PMCID: PMC3942319
- DOI: 10.1371/journal.pone.0088788
Th1 response and systemic treg deficiency in inclusion body myositis
Abstract
Objective: Sporadic inclusion body myositis (sIBM), the most frequent myositis in elderly patients, is characterized by the presence muscle inflammation and degeneration. We aimed at characterizing immune responses and regulatory T cells, considered key players in the maintenance of peripheral immune tolerance, in sIBM.
Methods: Serum and muscle tissue levels of 25 cytokines and phenotype of circulating immune cells were measured in 22 sIBM patients and compared with 22 healthy subjects. Cytokine data were analysed by unsupervised hierarchical clustering and principal components analysis.
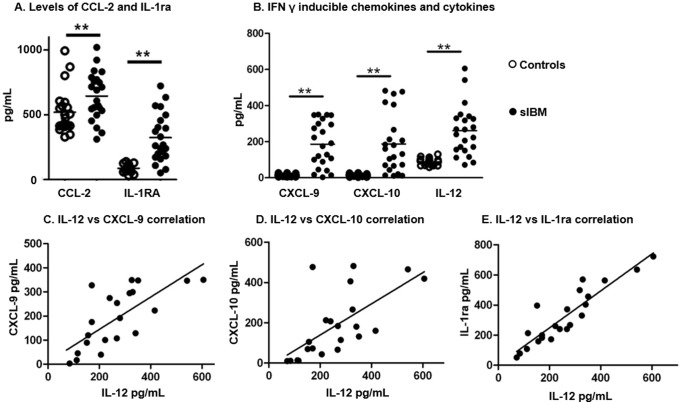
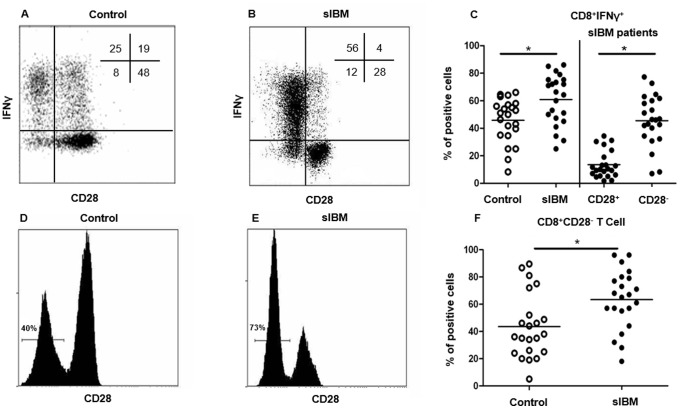
Results: Compared to healthy controls, sIBM patients had increased levels of Th-1 cytokines and chemokines such as IL-12 (261±138 pg/mL vs. 88±19 pg/mL; p<0.0001), CXCL-9 (186±12 pg/mL vs. 13±7 pg/mL; p<0.0001), and CXCL-10 (187±62 pg/mL vs. 13±6 pg/mL; p<0.0001). This was associated with an increased frequency of CD8+CD28- T cells (45.6±18.5% vs. 13.5±9.9%; p<0.0001), which were more prone to produce IFN-γ (45.6±18.5% vs. 13.5±9.9%; p<0.0001). sIBM patients also had a decreased frequency of circulating regulatory T cells (CD4+CD25+CD127lowFOXP3+, 6.9±1.7%; vs. 5.2±1.1%, p = 0.01), which displayed normal suppressor function and were also present in affected muscle.
Conclusion: sIBM patients present systemic immune activation with Th1 polarization involving the IFN-γ pathway and CD8+CD28- T cells associated with peripheral regulatory T cell deficiency.
Conflict of interest statement
Figures



References
-
- Benveniste O, Guiguet M, Freebody J, Dubourg O, Squier W, et al. (2011) Long-term observational study of sporadic body inclusion body myositis. Brain 134(Pt11): 3176–84. - PubMed
-
- Dimitri D, Benveniste O, Dubourg O, Maisonobe T, Eymard B, et al. (2006) Shared blood and muscle CD8+ T-cell expansions in inclusion body myositis. Brain, 129(Pt 4): 986–995. - PubMed
-
- Griggs RC, Askanas V, DiMauro S, Engel A, Karpati G, et al. (1995) Inclusion body myositis and myopathies. Ann Neurol 38(5): 705–713. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
