

Delay from first medical contact to primary PCI and all-cause mortality: a nationwide study of patients with ST-elevation myocardial infarction
- PMID: 24595190
- PMCID: PMC4187473
- DOI: 10.1161/JAHA.113.000486
Delay from first medical contact to primary PCI and all-cause mortality: a nationwide study of patients with ST-elevation myocardial infarction
Abstract
Background: Early reperfusion in the setting of an ST-elevation myocardial infarction (STEMI) is of utmost importance. However, the effects of early versus late reperfusion in this patient group undergoing primary percutaneous coronary intervention (PCI) have so far been inconsistent in previous studies. The purpose of this study was to evaluate in a nationwide cohort the effects of delay from first medical contact to PCI (first medical contact [FMC]-to-PCI) and secondarily delay from symptom-to-PCI on clinical outcomes.
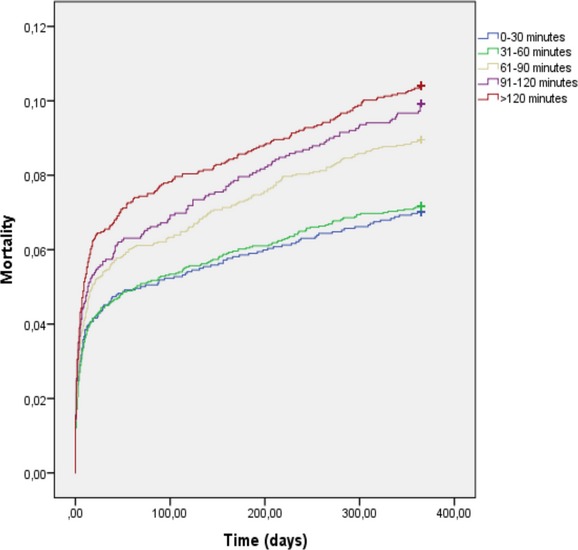
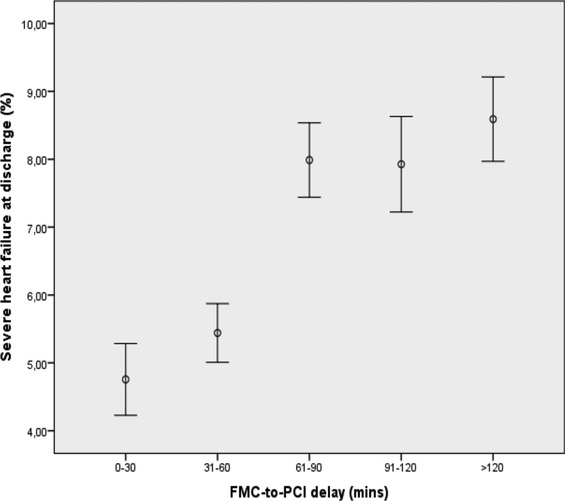
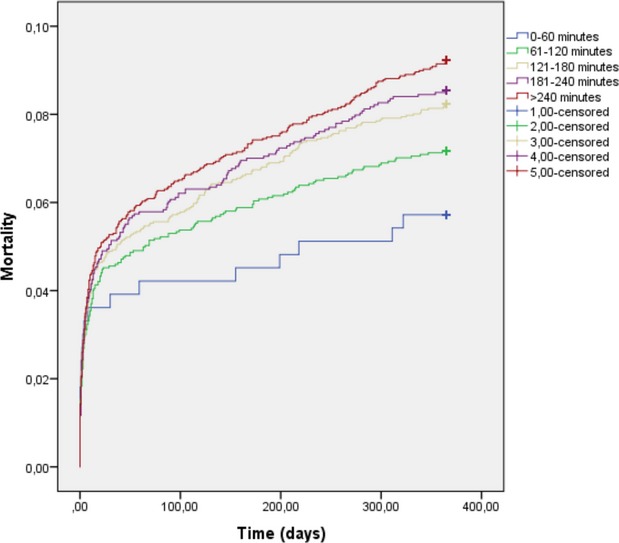
Methods and results: Using the national Swedish Coronary Angiography and Angioplasty Register (SCAAR) registry, STEMI patients undergoing primary PCI between the years 2003 and 2008 were screened for. A total of 13 790 patients were included in the FMC-to-PCI analysis and 11 489 patients were included in the symptom-to-PCI analyses. Unadjusted as well as multivariable analyses showed an overall significant association between increasing FMC-to-PCI delay and 1-year mortality. A statistically significant increase in mortality was noted at FMC-to-PCI delays exceeding 1 hour in an incremental fashion. FMC-to-PCI delays in excess of 1 hour were also significantly associated with an increase in severe left ventricular dysfunction at discharge. An overall significant association between increasing symptom-to-PCI delays and 1-year mortality was noted. However, when stratified into time delay cohorts, no symptom-to-PCI delay except for the highest time delay showed a statistically significant association with increased mortality.
Conclusions: Delays in FMC-to-PCI were strongly associated with increased mortality already at delays of more than 1 hour, possibly through an increase in severe heart failure. A goal of FMC-to-PCI of less than 1 hour might save patient lives.
Keywords: ST‐segment elevation myocardial infarction; percutaneous coronary intervention.
Figures
References
-
- Steg PG, James SK, Atar D, Badano LP, Lundqvist CB, Borger MA, Di Mario C, Dickstein K, Ducrocq G, Fernandez‐Aviles F, Gershlick AH, Giannuzzi P, Halvorsen S, Huber K, Juni P, Kastrati A, Knuuti J, Lenzen MJ, Mahaffey KW, Valgimigli M, Van't Hof A, Widimsky P, Zahger D, Bax JJ, Baumgartner H, Ceconi C, Dean V, Deaton C, Fagard R, Funck‐Brentano C, Hasdai D, Hoes A, Kirchhof P, Kolh P, McDonagh T, Moulin C, Popescu BA, Reiner Z, Sechtem U, Sirnes PA, Tendera M, Torbicki A, Vahanian A, Windecker S, Astin F, Astrom‐Olsson K, Budaj A, Clemmensen P, Collet JP, Fox KA, Fuat A, Gustiene O, Hamm CW, Kala P, Lancellotti P, Maggioni AP, Merkely B, Neumann FJ, Piepoli MF, Van de Werf F, Verheugt F, Wallentin L. ESC guidelines for the management of acute myocardial infarction in patients presenting with ST‐segment elevation: the task force on the management of ST‐segment elevation acute myocardial infarction of the European Society of Cardiology (ESC). Eur Heart J. 2012; 33:2569-2619 - PubMed
-
- Schomig A, Ndrepepa G, Mehilli J, Schwaiger M, Schuhlen H, Nekolla S, Pache J, Martinoff S, Bollwein H, Kastrati A. Therapy‐dependent influence of time‐to‐treatment interval on myocardial salvage in patients with acute myocardial infarction treated with coronary artery stenting or thrombolysis. Circulation. 2003; 108:1084-1088 - PubMed
-
- Thiele H, Kappl MJ, Linke A, Erbs S, Boudriot E, Lembcke A, Kivelitz D, Schuler G. Influence of time‐to‐treatment, TIMI‐flow grades, and ST‐segment resolution on infarct size and infarct transmurality as assessed by delayed enhancement magnetic resonance imaging. Eur Heart J. 2007; 28:1433-1439 - PubMed
-
- Prehospital thrombolytic therapy in patients with suspected acute myocardial infarction. The European Myocardial Infarction Project Group. N Engl J Med. 1993; 329:383-389 - PubMed
-
- Morrison LJ, Verbeek PR, McDonald AC, Sawadsky BV, Cook DJ. Mortality and prehospital thrombolysis for acute myocardial infarction: a meta‐analysis. JAMA. 2000; 283:2686-2692 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
