

Seizure burden is independently associated with short term outcome in critically ill children
- PMID: 24595203
- PMCID: PMC3999716
- DOI: 10.1093/brain/awu042
Seizure burden is independently associated with short term outcome in critically ill children
Abstract
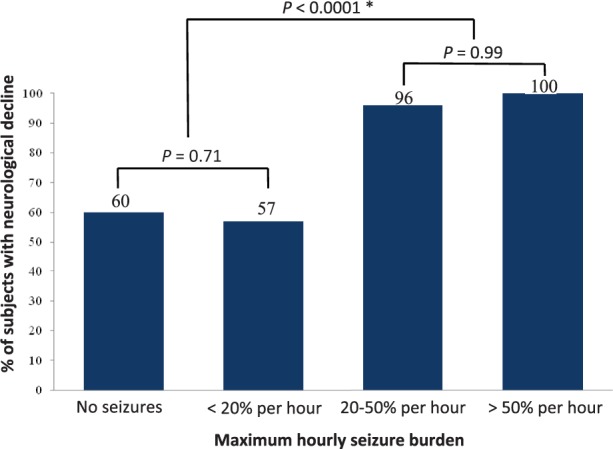
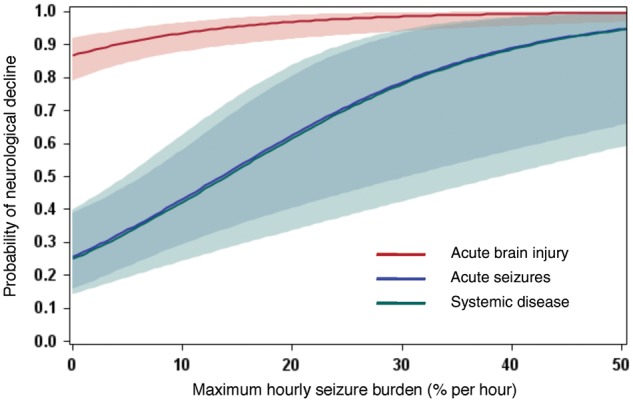
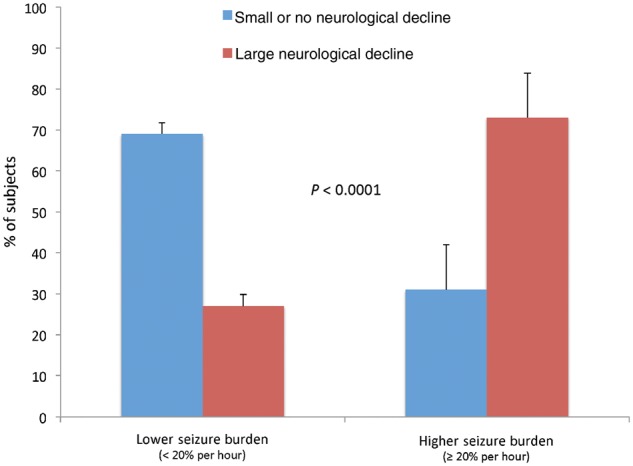
Seizures are common among critically ill children, but their relationship to outcome remains unclear. We sought to quantify the relationship between electrographic seizure burden and short-term neurological outcome, while controlling for diagnosis and illness severity. Furthermore, we sought to determine whether there is a seizure burden threshold above which there is an increased probability of neurological decline. We prospectively evaluated all infants and children admitted to our paediatric and cardiac intensive care units who underwent clinically ordered continuous video-electroencephalography monitoring over a 3-year period. Seizure burden was quantified by calculating the maximum percentage of any hour that was occupied by electrographic seizures. Outcome measures included neurological decline, defined as a worsening Paediatric Cerebral Performance Category score between hospital admission and discharge, and in-hospital mortality. Two hundred and fifty-nine subjects were evaluated (51% male) with a median age of 2.2 years (interquartile range: 0.3 days-9.7 years). The median duration of continuous video-electroencephalography monitoring was 37 h (interquartile range: 21-56 h). Seizures occurred in 93 subjects (36%, 95% confidence interval = 30-42%), with 23 (9%, 95% confidence interval = 5-12%) experiencing status epilepticus. Neurological decline was observed in 174 subjects (67%), who had a mean maximum seizure burden of 15.7% per hour, compared to 1.8% per hour for those without neurological decline (P < 0.0001). Above a maximum seizure burden threshold of 20% per hour (12 min), both the probability and magnitude of neurological decline rose sharply (P < 0.0001) across all diagnostic categories. On multivariable analysis adjusting for diagnosis and illness severity, the odds of neurological decline increased by 1.13 (95% confidence interval = 1.05-1.21, P = 0.0016) for every 1% increase in maximum hourly seizure burden. Seizure burden was not associated with mortality (odds ratio: 1.003, 95% confidence interval: 0.99-1.02, P = 0.613). We conclude that in this cohort of critically ill children, increasing seizure burden was independently associated with a greater probability and magnitude of neurological decline. Our observation that a seizure burden of more than 12 min in a given hour was strongly associated with neurological decline suggests that early antiepileptic drug management is warranted in this population, and identifies this seizure burden threshold as a potential therapeutic target. These findings support the hypothesis that electrographic seizures independently contribute to brain injury and worsen outcome. Our results motivate and inform the design of future studies to determine whether more aggressive seizure treatment can improve outcome.
Keywords: child; continuous video-EEG monitoring; critical illness; outcome; seizure burden.
Figures

Comment in
-
To know or not to know: does EEG monitoring in the paediatric intensive care unit add anything besides cost?Brain. 2014 May;137(Pt 5):1276-7. doi: 10.1093/brain/awu080. Brain. 2014. PMID: 24771398 Free PMC article. No abstract available.
-
Reply: The circular dilemma of seizure-induced brain injury.Brain. 2014 Nov;137(Pt 11):e306. doi: 10.1093/brain/awu186. Epub 2014 Jul 3. Brain. 2014. PMID: 24993960 Free PMC article. No abstract available.
-
The circular dilemma of seizure-induced brain injury.Brain. 2014 Nov;137(Pt 11):e305. doi: 10.1093/brain/awu185. Epub 2014 Jul 3. Brain. 2014. PMID: 24993961 No abstract available.
References
-
- Brophy GM, Bell R, Claassen J, Alldredge B, Bleck TP, Glauser T, et al. Guidelines for the evaluation and management of status epilepticus. Neurocrit Care. 2012;17:3–23. - PubMed
-
- Carrera E, Claassen J, Oddo M, Emerson RG, Mayer SA, Hirsch LJ. Continuous electroencephalographic monitoring in critically ill patients with central nervous system infections. Arch Neurol. 2008;65:1612–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
