

Envisioning the next WHO head and neck classification
- PMID: 24595418
- PMCID: PMC3950391
- DOI: 10.1007/s12105-014-0529-5
Envisioning the next WHO head and neck classification
Abstract
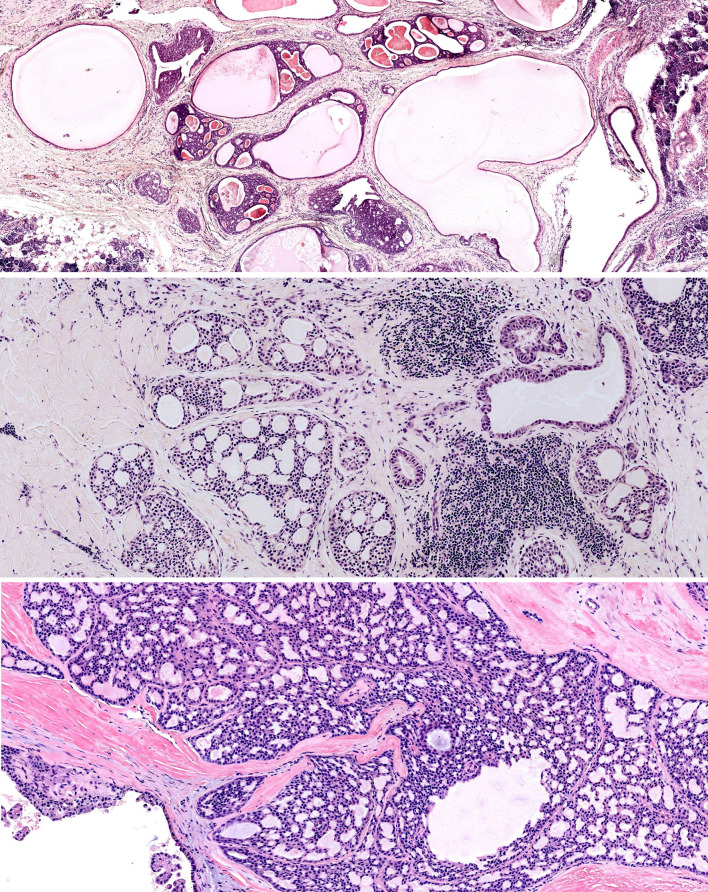
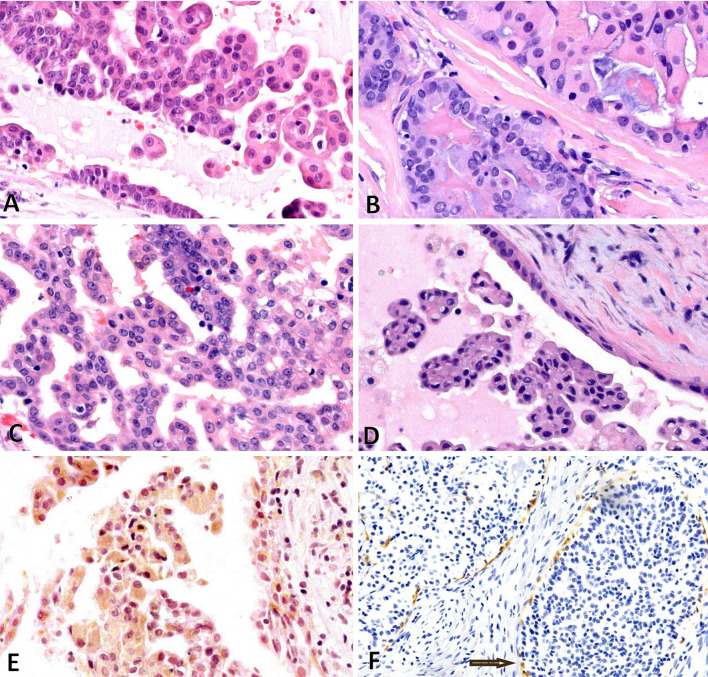
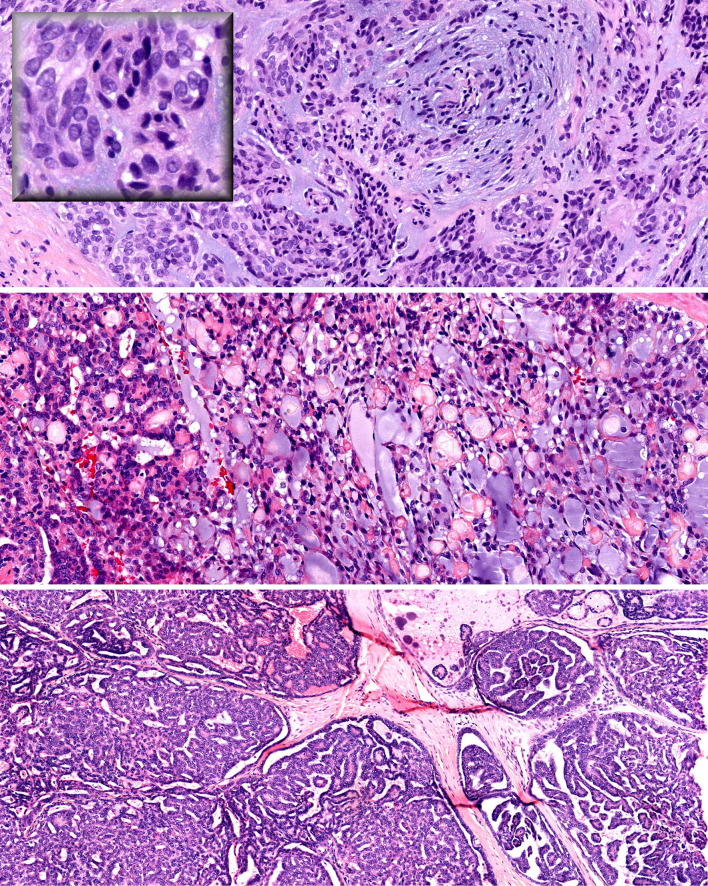
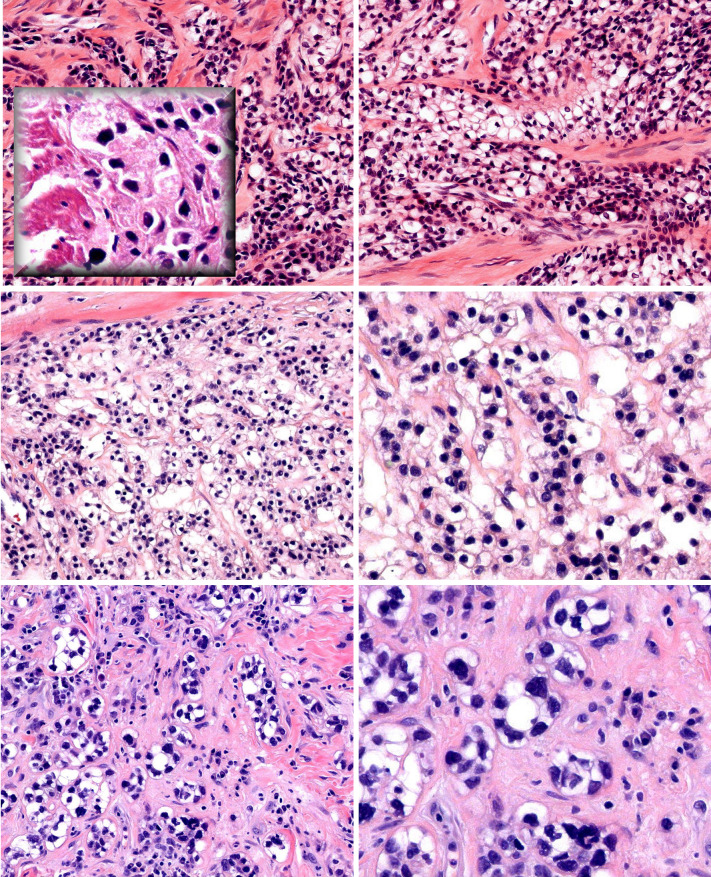
The next WHO classification should abandon "salivary duct carcinoma"; conventional salivary duct carcinoma should be classified as "high-grade salivary duct carcinoma". Low-grade salivary duct carcinoma should replace the current nosology of "low-grade cribriform cystadenocarcinoma". Cystadenocarcinoma should be classified with the descriptor "Not Otherwise Specified" and should be considered an exclusionary diagnostic category. On the other hand, "Not Otherwise Specified" does not fit for hyalinizing clear cell carcinoma (HCCC). The EWSR1-ATF1 fusion is specific for HCCC within the context of salivary neoplasia. We recommend adding "hyalinizing" even though this feature is not present in all cases; the benefit of which is the mental association with a salivary clear cell malignancy. Sinonasal Renal Cell-like Adenocarcinoma (SNRCLA) is a distinct clear cell neoplasm and should be added to the next WHO classification. Future studies will bear out whether SNRCLA is even a low-grade carcinoma, or may be reclassified as "adenoma". Lastly, the next WHO monograph should include the Risk Model in the general introductory statements on oral squamous cell carcinoma, under a subheading of "Histological Prognosticators". The positive predictive value for developing locoregional recurrence in patients with low-stage oral cavity squamous carcinoma (OSCC) and "worst pattern of invasion type-5" (WPOI-5) is 42 %. Low-stage high-risk OSCC with a combination of features other than WPOI-5 is associated with 32 % likelihood for locoregional progression. WPOI-5 also predicts occult metastatic disease (p = 0.0001, Chi squared, 2 DF). Thus the Risk Model can also be used to make decisions regarding staged elective neck dissections.
Figures



References
-
- Brandwein-Gensler M, Hille J, Wang BY, Urken M, Gordon R, Wang LJ, Simpson JR, Simpson RH, Gnepp DR. Low-grade salivary duct carcinoma: description of 16 cases. Am J Surg Pathol. 2004;28:1040–1044. doi: 10.1097/01.pas.0000128662.66321.be. - DOI - PubMed
-
- Brandwein-Gensler M, Gnepp DR, et al. Low-grade cribriform cystadenocarcinoma. In: Barnes L, Eveson JW, Reichart P, et al., editors. Pathology and genetics head and neck tumors. Lyon: IARC Press; 2005. p. 233.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
