

doi: 10.1007/s12105-014-0533-9.
Epub 2014 Mar 5.
Recently described sinonasal tract lesions/neoplasms: considerations for the new world health organization book
Affiliations
- PMID: 24595422
- PMCID: PMC3950390
- DOI: 10.1007/s12105-014-0533-9
Item in Clipboard
Recently described sinonasal tract lesions/neoplasms: considerations for the new world health organization book
Head Neck Pathol.
2014 Mar.
Abstract
Since the publication of the World Health Organization Classification of Head and Neck Tumors (Barnes et al., World Health Organization classification of tumours. Pathology and genetics head and neck tumours, IARC Press, Lyon, pp 10-80, 2001), a number of sinonasal lesions have been more completely described. This manuscript will focus on three such "new" lesions including sero mucinous hamartoma, HPV-related carcinoma with adenoid cystic-like features and low-grade sinonasal sarcoma with neural and myogenic features.
Figures
a, b. Seromucinous hamartoma characterized by the presence of a submucosal epithelial proliferation of small glands, serous acini and tubules growing in clusters and lobules; c in areas the glands may be densely packed with a back-to-back (cribriform) appearance that may suggest a possible diagnosis of an adenocarcinoma. d Invagination of the surface respiratory epithelium may be seen (arrows) that in conjunction with periglandular hyalinization are features seen in the READ hamartoma. These histologic features in conjunction with the submucosal seromucinous glandular proliferation that typify features of SH raise the notion that SH and READ hamartoma represent a spectrum of the same lesion rather than different lesions

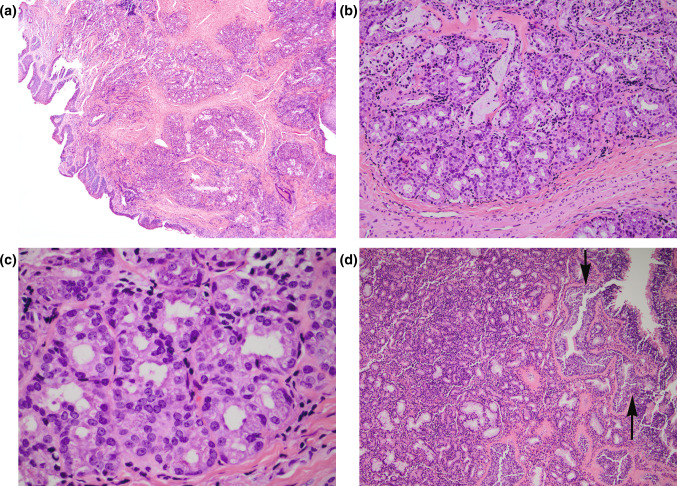
Human papillomavirus-related carcinoma with adenoid cystic-like features. a The histologic features include the presence of an invasive hypercellular lesion with solid, lobular and nested growth separated by fibrous stroma. Mixed growth patterns seen include: b cribriform, c microcystic, and d true ductal structures, the latter representing a minor component. The microcystic spaces are filled with basophilic appearing material. The neoplastic infiltrate is predominantly comprised of basaloid cells with hyperchromatic and angulated nuclei while the true duct cells appear cuboidal with eosinophilic cytoplasm often located at center of lobules surrounded by zones of basaloid cells. e Intraepithelial dysplasia of the surface epithelium is present in a majority of cases. f. Strong and diffuse p16 reactivity (nuclear and cytoplasmic) is present
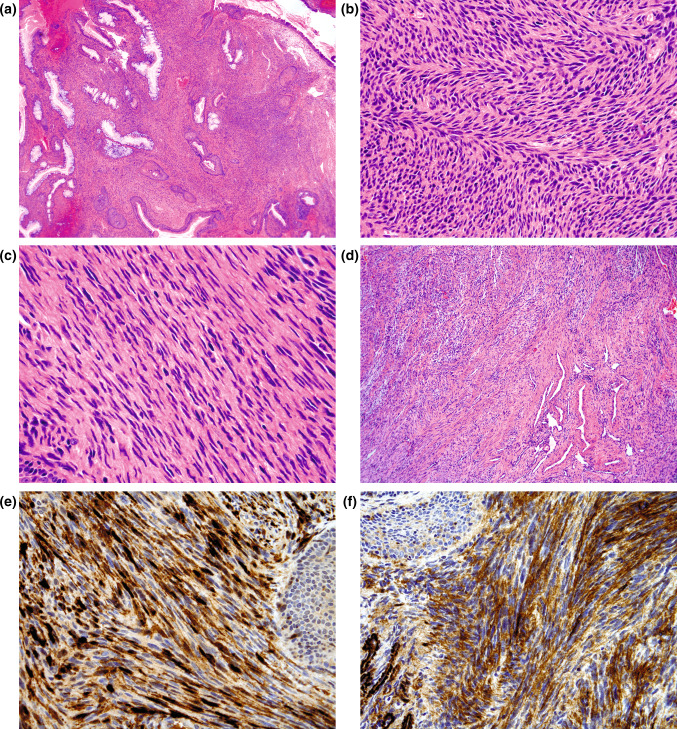
Low-grade sinonasal sarcoma with neural and myogenic differentiation. a Polypoid appearing sinonasal mucosa showing a poorly circumscribed and unencapsulated submucosal cellular spindle cell proliferation intimately associated with variably sized benign glands invaginating from the surface respiratory epithelium; b most examples show foci of classic “herringbone” pattern; c wavy to buckled appearing nuclei may be focally identified. Despite the hypercellularity, the tumor cells are highly uniform lacking significant nuclear pleomorphism and increased mitotic activity; d a hemangiopericytomatous vascular pattern may also be present; immunohistochemical staining shows the lesional cells to be reactive for e S100 protein (diffuse and strong) and f muscle specific actin
References
-
- Barnes L, Eveson JW, Reichart P, Sidransky D. Tumours of the nasal cavity and paranasal sinuses. In: Barnes L, Eveson JW, Reichart P, Sidransky D, editors. World Health Organization classification of tumours. Pathology and genetics head and neck tumours. IARC Press; Lyon: 2005:10–80.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
