

Treatment of psoriatic arthritis in a phase 3 randomised, placebo-controlled trial with apremilast, an oral phosphodiesterase 4 inhibitor
- PMID: 24595547
- PMCID: PMC4033106
- DOI: 10.1136/annrheumdis-2013-205056
Treatment of psoriatic arthritis in a phase 3 randomised, placebo-controlled trial with apremilast, an oral phosphodiesterase 4 inhibitor
Abstract
Objectives: Apremilast, an oral phosphodiesterase 4 inhibitor, regulates inflammatory mediators. Psoriatic Arthritis Long-term Assessment of Clinical Efficacy 1 (PALACE 1) compared apremilast with placebo in patients with active psoriatic arthritis despite prior traditional disease-modifying antirheumatic drug (DMARD) and/or biologic therapy.
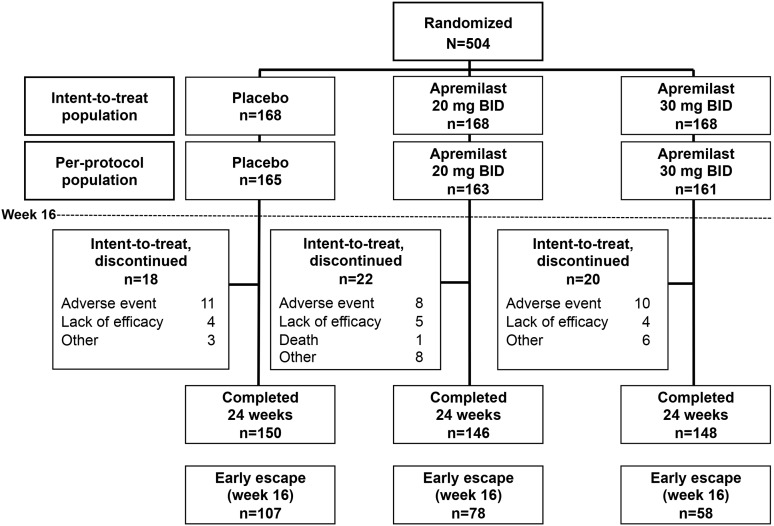
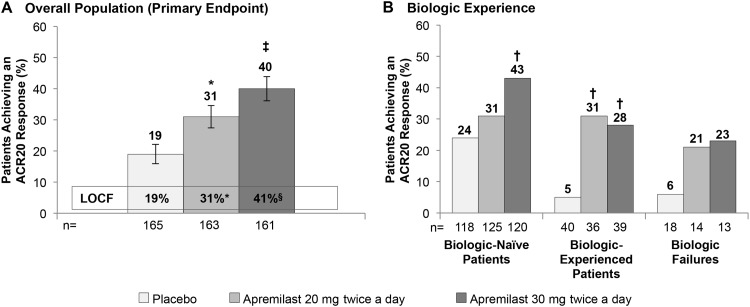
Methods: In the 24-week, placebo-controlled phase of PALACE 1, patients (N=504) were randomised (1:1:1) to placebo, apremilast 20 mg twice a day (BID) or apremilast 30 mg BID. At week 16, patients without ≥20% reduction in swollen and tender joint counts were required to be re-randomised equally to either apremilast dose if initially randomised to placebo or remained on their initial apremilast dose. Patients on background concurrent DMARDs continued stable doses (methotrexate, leflunomide and/or sulfasalazine). Primary outcome was the proportion of patients achieving 20% improvement in modified American College of Rheumatology response criteria (ACR20) at week 16.
Results: At week 16, significantly more apremilast 20 mg BID (31%) and 30 mg BID (40%) patients achieved ACR20 versus placebo (19%) (p<0.001). Significant improvements in key secondary measures (physical function, psoriasis) were evident with both apremilast doses versus placebo. Across outcome measures, the 30-mg group generally had higher and more consistent response rates, although statistical comparison was not conducted. The most common adverse events were gastrointestinal and generally occurred early, were self-limiting and infrequently led to discontinuation. No imbalance in major adverse cardiac events, serious or opportunistic infections, malignancies or laboratory abnormalities was observed.
Conclusions: Apremilast was effective in the treatment of psoriatic arthritis, improving signs and symptoms and physical function. Apremilast demonstrated an acceptable safety profile and was generally well tolerated.
Clinical trial registration number: NCT01172938.
Keywords: Psoriatic Arthritis; Spondyloarthritis; Treatment.
Figures
References
-
- Ash Z, Gaujoux-Viala C, Gossec L, et al. A systematic literature review of drug therapies for the treatment of psoriatic arthritis: current evidence and meta-analysis informing the EULAR recommendations for the management of psoriatic arthritis. Ann Rheum Dis 2012;71:319–26 - PubMed
-
- Gossec L, Smolen JS, Gaujoux-Viala C, et al. European League Against Rheumatism recommendations for the management of psoriatic arthritis with pharmacological therapies. Ann Rheum Dis 2012;71:4–12 - PubMed
-
- Menter A, Korman NJ, Elmets CA, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 4. Guidelines of care for the management and treatment of psoriasis with traditional systemic agents. J Am Acad Dermatol 2009;61:451–85 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
