

Outcomes of combined cardiovascular risk factor management strategies in type 2 diabetes: the ACCORD randomized trial
- PMID: 24595629
- PMCID: PMC4030092
- DOI: 10.2337/dc13-2334
Outcomes of combined cardiovascular risk factor management strategies in type 2 diabetes: the ACCORD randomized trial
Abstract
Objective: To compare effects of combinations of standard and intensive treatment of glycemia and either blood pressure (BP) or lipids in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial.
Research design and methods: ACCORD enrolled 10,251 type 2 diabetes patients aged 40-79 years at high risk for cardiovascular disease (CVD) events. Participants were randomly assigned to hemoglobin A1c goals of <6.0% (<42 mmol/mol; intensive glycemia) or 7.0-7.9% (53-63 mmol/mol; standard glycemia) and then randomized a second time to either 1) systolic BP goals of <120 mmHg (intensive BP) or <140 mmHg (standard BP) or 2) simvastatin plus fenofibrate (intensive lipid) or simvastatin plus placebo (standard lipid). Proportional hazards models were used to assess combinations of treatment assignments on the composite primary (deaths due to CVD, nonfatal myocardial infarction [MI], and nonfatal stroke) and secondary outcomes.
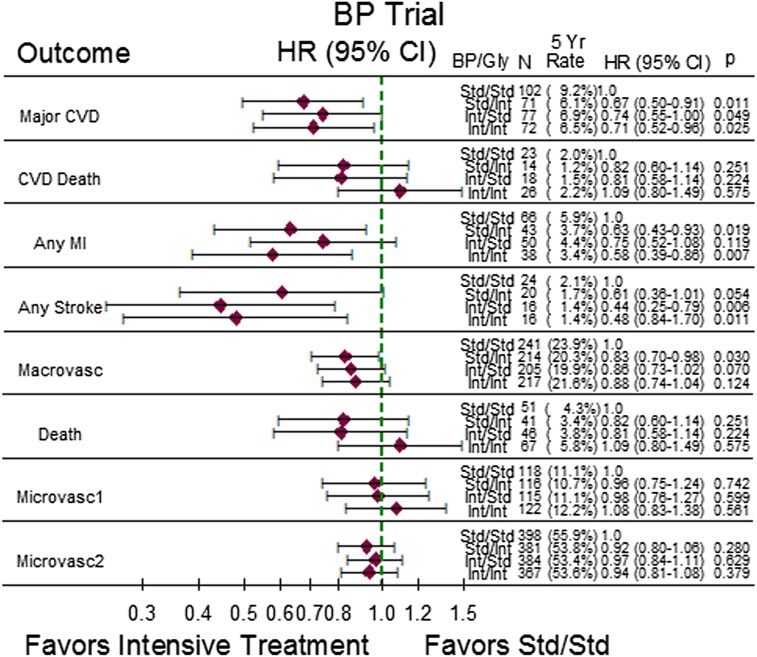
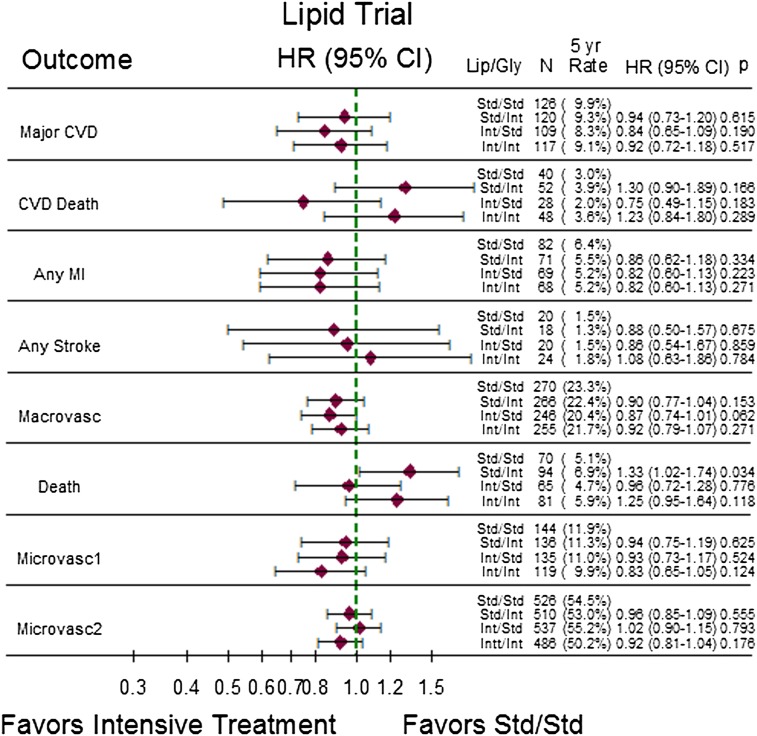
Results: In the BP trial, risk of the primary outcome was lower in the groups intensively treated for glycemia (hazard ratio [HR] 0.67; 95% CI 0.50-0.91), BP (HR 0.74; 95% CI 0.55-1.00), or both (HR 0.71; 95% CI 0.52-0.96) compared with combined standard BP and glycemia treatment. For secondary outcomes, MI was significantly reduced by intensive glycemia treatment and stroke by intensive BP treatment; most other HRs were neutral or favored intensive treatment groups. In the lipid trial, the general pattern of results showed no evidence of benefit of intensive regimens (whether single or combined) compared with combined standard lipid and glycemia treatment. The mortality HR was 1.33 (95% CI 1.02-1.74) in the standard lipid/intensive glycemia group compared with the standard lipid/standard glycemia group.
Conclusions: In the ACCORD BP trial, compared with combined standard treatment, intensive BP or intensive glycemia treatment alone improved major CVD outcomes, without additional benefit from combining the two. In the ACCORD lipid trial, neither intensive lipid nor glycemia treatment produced an overall benefit, but intensive glycemia treatment increased mortality.
Trial registration: ClinicalTrials.gov NCT00000620.
© 2014 by the American Diabetes Association.
Figures
References
-
- Stamler J, Vaccaro O, Neaton JD, Wentworth D. Diabetes, other risk factors, and 12-yr cardiovascular mortality for men screened in the Multiple Risk Factor Intervention Trial. Diabetes Care 1993;16:434–444 - PubMed
-
- Kearney PM, Blackwell L, Collins R, et al. Cholesterol Treatment Trialists’ (CTT) Collaborators Efficacy of cholesterol-lowering therapy in 18,686 people with diabetes in 14 randomised trials of statins: a meta-analysis. Lancet 2008;371:117–125 - PubMed
-
- Turnbull F, Neal B, Algert C, et al. Blood Pressure Lowering Treatment Trialists’ Collaboration Effects of different blood pressure-lowering regimens on major cardiovascular events in individuals with and without diabetes mellitus: results of prospectively designed overviews of randomized trials. Arch Intern Med 2005;165:1410–1419 - PubMed
-
- Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med 2008;359:1577–1589 - PubMed
-
- Gaede P, Lund-Andersen H, Parving HH, Pedersen O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med 2008;358:580–591 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
