

A higher-complex carbohydrate diet in gestational diabetes mellitus achieves glucose targets and lowers postprandial lipids: a randomized crossover study
- PMID: 24595632
- PMCID: PMC3994935
- DOI: 10.2337/dc13-2411
A higher-complex carbohydrate diet in gestational diabetes mellitus achieves glucose targets and lowers postprandial lipids: a randomized crossover study
Abstract
Objective: The conventional diet approach to gestational diabetes mellitus (GDM) advocates carbohydrate restriction, resulting in higher fat (HF), also a substrate for fetal fat accretion and associated with maternal insulin resistance. Consequently, there is no consensus about the ideal GDM diet. We hypothesized that, compared with a conventional, lower-carbohydrate/HF diet (40% carbohydrate/45% fat/15% protein), consumption of a higher-complex carbohydrate (HCC)/lower-fat (LF) Choosing Healthy Options in Carbohydrate Energy (CHOICE) diet (60/25/15%) would result in 24-h glucose area under the curve (AUC) profiles within therapeutic targets and lower postprandial lipids.
Research design and methods: Using a randomized, crossover design, we provided 16 GDM women (BMI 34 ± 1 kg/m2) with two 3-day isocaloric diets at 31 ± 0.5 weeks (washout between diets) and performed continuous glucose monitoring. On day 4 of each diet, we determined postprandial (5 h) glucose, insulin, triglycerides (TGs), and free fatty acids (FFAs) following a controlled breakfast meal.
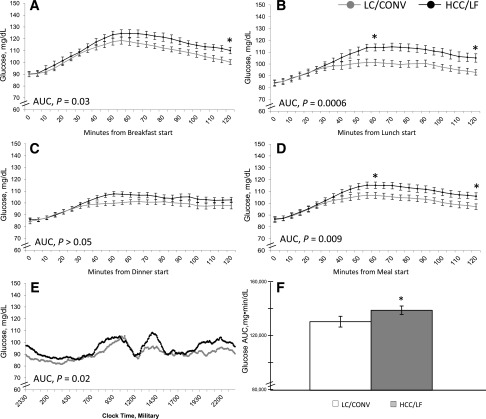
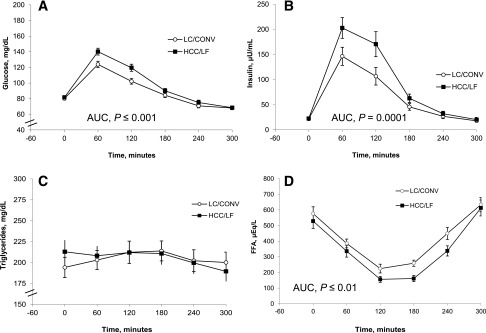
Results: There were no between-diet differences for fasting or mean nocturnal glucose, but 24-h AUC was slightly higher (∼6%) on the HCC/LF CHOICE diet (P = 0.02). The continuous glucose monitoring system (CGMS) revealed modestly higher 1- and 2-h postprandial glucose on CHOICE (1 h, 115 ± 2 vs. 107 ± 3 mg/dL, P ≤ 0.01; 2 h, 106 ± 3 vs. 97 ± 3 mg/dL, P = 0.001) but well below current targets. After breakfast, 5-h glucose and insulin AUCs were slightly higher (P < 0.05), TG AUC was no different, but the FFA AUC was significantly lower (∼19%; P ≤ 0.01) on the CHOICE diet.
Conclusions: This highly controlled study randomizing isocaloric diets and using a CGMS is the first to show that liberalizing complex carbohydrates and reducing fat still achieved glycemia below current treatment targets and lower postprandial FFAs. This diet strategy may have important implications for preventing macrosomia.
Figures
References
-
- Metzger BE, Buchanan TA, Coustan DR, et al. Summary and recommendations of the Fifth International Workshop-Conference on Gestational Diabetes Mellitus. Diabetes Care 2007;30(Suppl. 2):S251–S260 - PubMed
-
- Metzger BE, Gabbe SG, Persson B, et al. International Association of Diabetes and Pregnancy Study Groups Consensus Panel International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010;33:676–682 - PMC - PubMed
-
- Sacks DA, Hadden DR, Maresh M, et al. HAPO Study Cooperative Research Group Frequency of gestational diabetes mellitus at collaborating centers based on IADPSG consensus panel-recommended criteria: the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) Study. Diabetes Care 2012;35:526–528 - PMC - PubMed
-
- National Institutes of Health. National Institutes of Health Consensus Development Conference: Diagnosing Gestational Diabetes Mellitus, 2013. Available from http://prevention.nih.gov/cdp/conferences/2013/gdm/resources.aspx
-
- Jovanovic-Peterson L, Peterson CM. Dietary manipulation as a primary treatment strategy for pregnancies complicated by diabetes. J Am Coll Nutr 1990;9:320–325 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
