

Associations of housing mobility interventions for children in high-poverty neighborhoods with subsequent mental disorders during adolescence
- PMID: 24595778
- PMCID: PMC4100467
- DOI: 10.1001/jama.2014.607
Associations of housing mobility interventions for children in high-poverty neighborhoods with subsequent mental disorders during adolescence
Retracted and republished in
-
Notice of Retraction and Replacement: Kessler RC, et al. Associations of Housing Mobility Interventions for Children in High-Poverty Neighborhoods With Subsequent Mental Disorders During Adolescence. JAMA. 2014;311(9):937-947.JAMA. 2016 Jul 12;316(2):227-8. doi: 10.1001/jama.2016.6187. JAMA. 2016. PMID: 27315194 Free PMC article. No abstract available.
Abstract
Importance: Youth in high-poverty neighborhoods have high rates of emotional problems. Understanding neighborhood influences on mental health is crucial for designing neighborhood-level interventions.
Objective: To perform an exploratory analysis of associations between housing mobility interventions for children in high-poverty neighborhoods and subsequent mental disorders during adolescence.
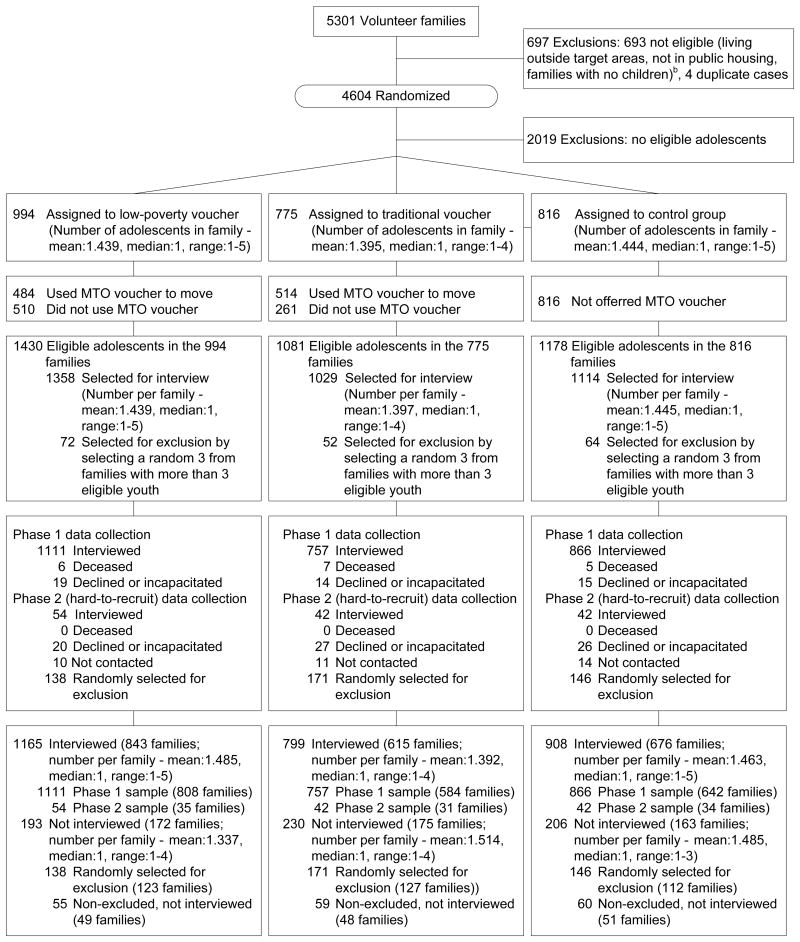
Design, setting, and participants: The Moving to Opportunity Demonstration from 1994 to 1998 randomized 4604 volunteer public housing families with 3689 children in high-poverty neighborhoods into 1 of 2 housing mobility intervention groups (a low-poverty voucher group vs a traditional voucher group) or a control group. The low-poverty voucher group (n=1430) received vouchers to move to low-poverty neighborhoods with enhanced mobility counseling. The traditional voucher group (n=1081) received geographically unrestricted vouchers. Controls (n=1178) received no intervention. Follow-up evaluation was performed 10 to 15 years later (June 2008-April 2010) with participants aged 13 to 19 years (0-8 years at randomization). Response rates were 86.9% to 92.9%.
Main outcomes and measures: Presence of mental disorders from the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition) within the past 12 months, including major depressive disorder, panic disorder, posttraumatic stress disorder (PTSD), oppositional-defiant disorder, intermittent explosive disorder, and conduct disorder, as assessed post hoc with a validated diagnostic interview.
Results: Of the 3689 adolescents randomized, 2872 were interviewed (1407 boys and 1465 girls). Compared with the control group, boys in the low-poverty voucher group had significantly increased rates of major depression (7.1% vs 3.5%; odds ratio (OR), 2.2 [95% CI, 1.2-3.9]), PTSD (6.2% vs 1.9%; OR, 3.4 [95% CI, 1.6-7.4]), and conduct disorder (6.4% vs 2.1%; OR, 3.1 [95% CI, 1.7-5.8]). Boys in the traditional voucher group had increased rates of PTSD compared with the control group (4.9% vs 1.9%, OR, 2.7 [95% CI, 1.2-5.8]). However, compared with the control group, girls in the traditional voucher group had decreased rates of major depression (6.5% vs 10.9%; OR, 0.6 [95% CI, 0.3-0.9]) and conduct disorder (0.3% vs 2.9%; OR, 0.1 [95% CI, 0.0-0.4]).
Conclusions and relevance: Interventions to encourage moving out of high-poverty neighborhoods were associated with increased rates of depression, PTSD, and conduct disorder among boys and reduced rates of depression and conduct disorder among girls. Better understanding of interactions among individual, family, and neighborhood risk factors is needed to guide future public housing policy changes.
Conflict of interest statement
Figures
Comment in
-
Socioeconomic influences on child health: building new ladders of social opportunity.JAMA. 2014 Mar 5;311(9):915-7. doi: 10.1001/jama.2014.608. JAMA. 2014. PMID: 24595774 No abstract available.
-
Housing mobility and adolescent mental health.JAMA. 2014 Jul;312(2):190. doi: 10.1001/jama.2014.6468. JAMA. 2014. PMID: 25005662 No abstract available.
-
Housing mobility and adolescent mental health--reply.JAMA. 2014 Jul;312(2):190-1. doi: 10.1001/jama.2014.6471. JAMA. 2014. PMID: 25005663 No abstract available.
References
-
- Leventhal T, Dupere V, Brooks-Gunn J. Neighborhood influences on adolescent development. In: Lerner RM, Steinberg L, editors. Handbook of Adolescent Psychology. Hoboken, NJ: Wiley; 2009. pp. 411–443.
-
- Galster GC. The mechanism(s) of neighborhood effects: Theory, evidence, and policy implications. In: van Ham M, Manley D, Bailey N, Simpson L, Maclennan D, editors. Neighborhood Effects Research: New Perspectives. New York: Springer; 2012. pp. 23–56.
-
- Diez Roux AV, Mair C. Neighborhoods and health. Ann N Y Acad Sci. 2010;1186:125–145. - PubMed
-
- Centers for Disease Control and Prevention. [Accessed May, 1 2013];Healthy Communities Program. 2013 http://www.cdc.gov/healthycommunitiesprogram/
Publication types
MeSH terms
Grants and funding
- R01 MH077026/MH/NIMH NIH HHS/United States
- R01 HD040404/HD/NICHD NIH HHS/United States
- P01-AG005842-22S1/AG/NIA NIH HHS/United States
- R01-HD040444/HD/NICHD NIH HHS/United States
- R01-AG031259/AG/NIA NIH HHS/United States
- P30 AG012810/AG/NIA NIH HHS/United States
- R49-CE000906/CE/NCIPC CDC HHS/United States
- R49 CE000906/CE/NCIPC CDC HHS/United States
- R01-MH077026/MH/NIMH NIH HHS/United States
- R24-HD051152-04/HD/NICHD NIH HHS/United States
- R01 HD040444/HD/NICHD NIH HHS/United States
- R24 HD051152/HD/NICHD NIH HHS/United States
- P01 AG005842/AG/NIA NIH HHS/United States
- R01 AG031259/AG/NIA NIH HHS/United States
- R01-HD040404/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
