

A multicenter randomized controlled trial of tonsillectomy combined with steroid pulse therapy in patients with immunoglobulin A nephropathy
- PMID: 24596084
- PMCID: PMC4106640
- DOI: 10.1093/ndt/gfu020
A multicenter randomized controlled trial of tonsillectomy combined with steroid pulse therapy in patients with immunoglobulin A nephropathy
Abstract
Background: The study aim was, for the first time, to conduct a multicenter randomized controlled trial to evaluate the effect of tonsillectomy in patients with IgA nephropathy (IgAN).
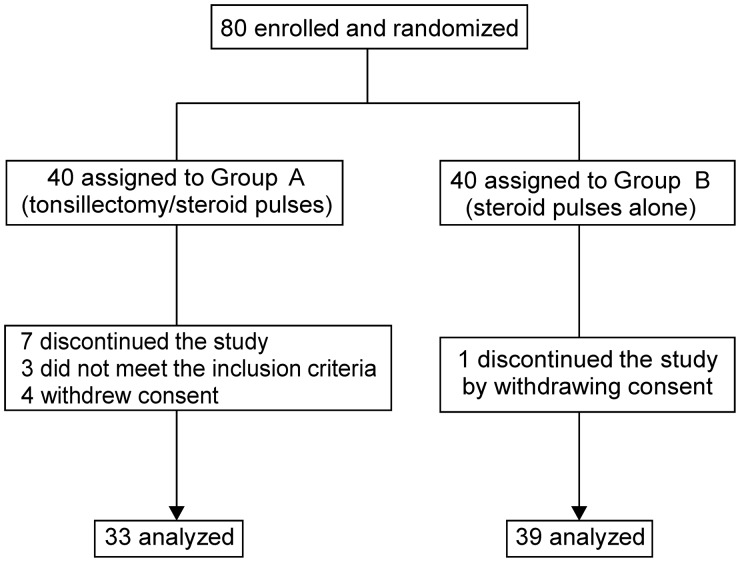
Methods: Patients with biopsy-proven IgAN, proteinuria and low serum creatinine were randomly allocated to receive tonsillectomy combined with steroid pulses (Group A; n = 33) or steroid pulses alone (Group B; n = 39). The primary end points were urinary protein excretion and the disappearance of proteinuria and/or hematuria.
Results: During 12 months from baseline, the percentage decrease in urinary protein excretion was significantly larger in Group A than that in Group B (P < 0.05). However, the frequency of the disappearance of proteinuria, hematuria, or both (clinical remission) at 12 months was not statistically different between the groups. Logistic regression analyses revealed the assigned treatment was a significant, independent factor contributing to the disappearance of proteinuria (odds ratio 2.98, 95% CI 1.01-8.83, P = 0.049), but did not identify an independent factor in achieving the disappearance of hematuria or clinical remission.
Conclusions: The results indicate tonsillectomy combined with steroid pulse therapy has no beneficial effect over steroid pulses alone to attenuate hematuria and to increase the incidence of clinical remission. Although the antiproteinuric effect was significantly greater in combined therapy, the difference was marginal, and its impact on the renal functional outcome remains to be clarified.
Keywords: clinical remission; estimated glomerular filtration rate; hematuria; proteinuria.
© The Author 2014. Published by Oxford University Press on behalf of ERA-EDTA.
Figures





References
-
- Koyama A, Igarashi M, Kobayashi M. Natural history and risk factors for immunoglobulin A nephropathy in Japan. Research Group on Progressive Renal Diseases. Am J Kidney Dis. 1997;29:526–532. - PubMed
-
- D'Amico G. Natural history of idiopathic IgA nephropathy: Role of clinical and histological prognostic factors. Am J Kidney Dis. 2000;36:227–237. - PubMed
-
- Nicholls KM, Fairley KF, Dowling JP, et al. The clinical course of mesangial IgA associated nephropathy in adults. Q J Med. 1984;53:227–250. - PubMed
-
- Beukhof JR, Kardaun O, Schaafsma W, et al. Toward individual prognosis of IgA nephropathy. Kindey Int. 1986;29:549–556. - PubMed
-
- Alamartine E, Sabatier JC, Guerin C, et al. Prognostic factors in mesangial IgA glomerulonephritis: An extensive study with univariate and multivariate analysis. Am J Kidney Dis. 1991;18:12–19. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
