

Percutaneous ablation of the small renal mass-techniques and outcomes
- PMID: 24596438
- PMCID: PMC3930659
- DOI: 10.1055/s-0033-1363841
Percutaneous ablation of the small renal mass-techniques and outcomes
Abstract
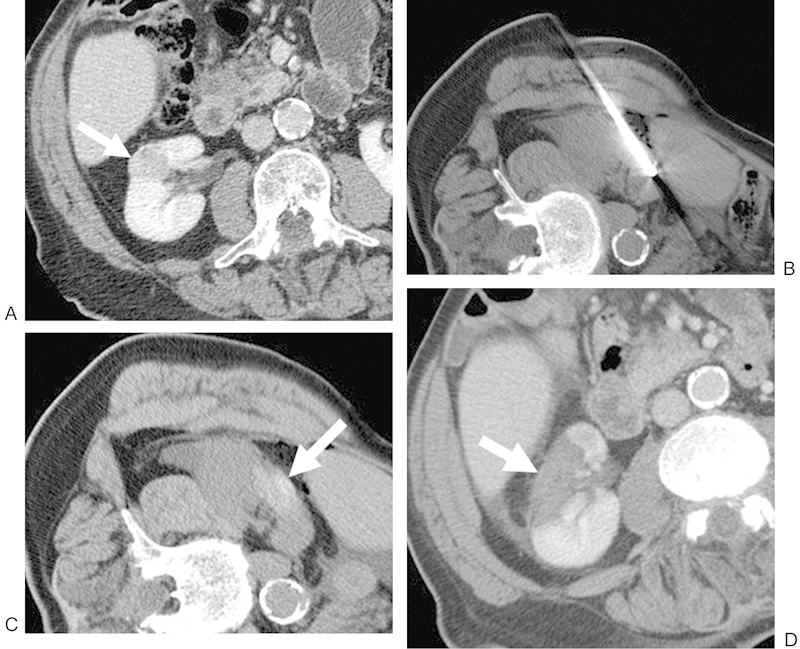
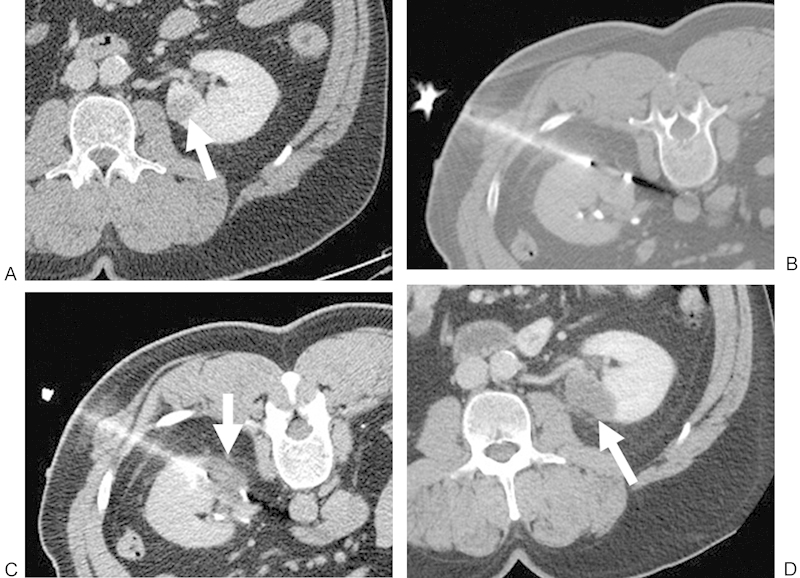
An increasing number of T1a renal cell carcinomas are being diagnosed in recent years, in part due to incidental detection from the increased use of cross-sectional imaging. Although partial nephrectomy is still considered the primary treatment for these small renal masses, percutaneous ablation is now being performed as a standard therapeutic, nephron-sparing approach in patients who are poor surgical candidates. Clinical studies to date have demonstrated that percutaneous ablation is an effective therapy with acceptable outcomes and low risk in the appropriate clinical settings. This article will review various clinical aspects regarding the percutaneous ablation of small renal masses, including patient selection, preprocedural preparations, and the procedural considerations of commonly employed ablative technologies. Specific techniques such as radiofrequency ablation, cryoablation, microwave ablation, irreversible electroporation, and high-intensity focused ultrasound will be addressed in detail. In addition, the technical and oncologic outcomes of percutaneous ablation will be discussed and referenced to that of partial nephrectomy.
Keywords: cryoablation; interventional radiology; percutaneous ablation; radiofrequency ablation; renal mass.
Figures

References
-
- National Cancer Institute. Kidney cancer home page Available at: http://www.cancer.gov/cancertopics/types/kidney. Accessed September 25, 2013
-
- Pantuck A J, Zisman A, Belldegrun A S. The changing natural history of renal cell carcinoma. J Urol. 2001;166(5):1611–1623. - PubMed
-
- Gervais D A, McGovern F J, Arellano R S, McDougal W S, Mueller P R. Radiofrequency ablation of renal cell carcinoma: part 1, indications, results, and role in patient management over a 6-year period and ablation of 100 tumors. AJR Am J Roentgenol. 2005;185(1):64–71. - PubMed
-
- Zagoria R J, Hawkins A D, Clark P E. et al.Percutaneous CT-guided radiofrequency ablation of renal neoplasms: factors influencing success. AJR Am J Roentgenol. 2004;183(1):201–207. - PubMed
-
- Jayson M, Sanders H. Increased incidence of serendipitously discovered renal cell carcinoma. Urology. 1998;51(2):203–205. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
