

Risk-adjusted survival after tissue versus mechanical aortic valve replacement: a 23-year assessment
- PMID: 24597402
- PMCID: PMC4348365
Risk-adjusted survival after tissue versus mechanical aortic valve replacement: a 23-year assessment
Abstract
Background and aim of the study: Detailed analyses of risk-adjusted outcomes after mitral valve surgery have documented significant survival decrements with tissue valves at any age. Several recent studies of prosthetic aortic valve replacement (AVR) also have suggested a poorer performance of tissue valves, although analyses have been limited to small matched series. The study aim was to test the hypothesis that AVR with tissue valves is associated with a lower risk-adjusted survival, as compared to mechanical valves.
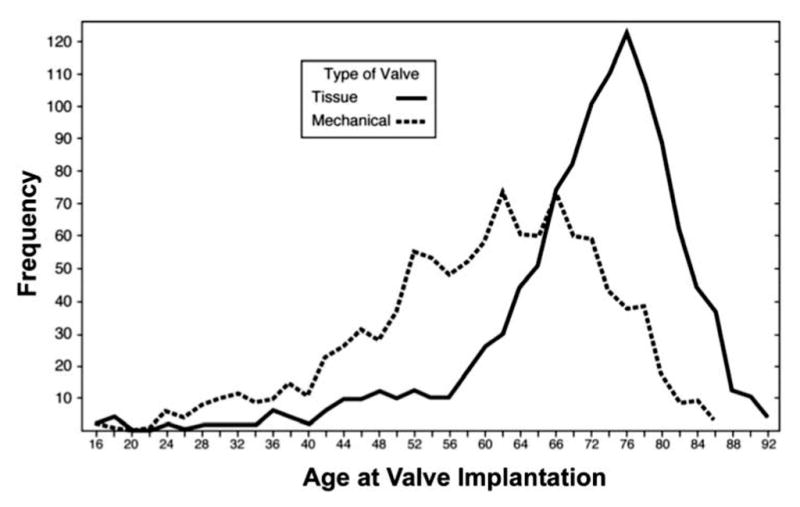
Methods: Between 1986 and 2009, primary isolated AVR, with or without coronary artery bypass grafting (CABG), was performed with currently available valve types in 2148 patients (1108 tissue valves, 1040 mechanical). Patients were selected for tissue valves to be used primarily in the elderly. Baseline and operative characteristics were documented prospectively with a consistent variable set over the entire 23-year period. Follow up was obtained with mailed questionnaires, supplemented by National Death Index searches. The average time to death or follow up was seven years, and follow up for survival was 96.2% complete. Risk-adjusted survival characteristics for the two groups were evaluated using a Cox proportional hazards model with stepwise selection of candidate variables.
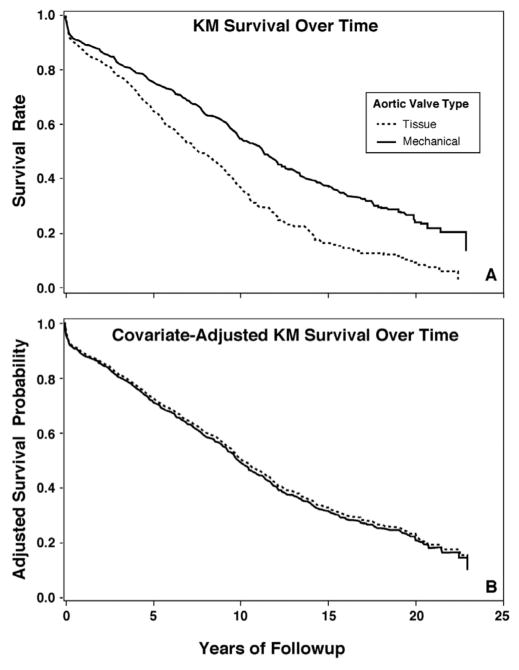
Results: Differences in baseline characteristics between groups were (tissue versus mechanical): median age 73 versus 61 years; non-elective surgery 32% versus 28%; CABG 45% versus 35%; median ejection fraction 55% versus 55%; renal failure 6% versus 1%; diabetes 18% versus 7% (p<0.01). Unadjusted Kaplan-Meier survival was significantly lower with tissue than mechanical valves; however, after risk adjustment for the adverse profiles of tissue valve patients, no significant difference was observed in survival after tissue or mechanical AVR. Thus, the hypothesis did not hold, and risk-adjusted survival was equivalent, of course qualified by the fact that selection bias was evident.
Conclusion: With selection criteria that employed tissue AVR more frequently in elderly patients, tissue and mechanical valves achieved similar survival characteristics across the spectrum of patient risk. Further studies of the relative outcomes of mechanical versus tissue valves across the spectrum of patient age seem indicated.
Figures
References
-
- Bonow RO, Carabello BA, Chatterjee K, et al. 2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients with valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;52:e1–e142. - PubMed
-
- Gammie JS, Sheng S, Griffith BP, et al. Trends in mitral valve surgery in the United States: Results from the Society of Thoracic Surgeons Adult Cardiac Database. Ann Thorac Surg. 2009;87:1431–1439. - PubMed
-
- Daneshmand MA, Milano CA, Rankin JS, et al. Mitral valve repair for degenerative disease: A 20-year experience. Ann Thorac Surg. 2009;88:1828–1837. - PubMed
-
- Brown JM, O’Brien SM, Wu C, Sikora JAH, Griffith BP, Gammie JS. Isolated aortic valve replacement in North America comprising 108,687 patients in 10 years: Changes in risks, valve types, and outcomes in the Society of Thoracic Surgeons National Database. J Thorac Cardiovasc Surg. 2009;137:82–90. - PubMed
-
- Hammermeister K, Sethi GK, Henderson WG, Grover FL, Oprian C, Rahimtoola SH. Outcomes 15 years after valve replacement with a mechanical versus a bioprosthetic valve: Final report of the Veterans Affairs randomized trial. J Am Coll Cardiol. 2000;36:1152–1158. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials