

Vital signs: improving antibiotic use among hospitalized patients
- PMID: 24598596
- PMCID: PMC4584728
Vital signs: improving antibiotic use among hospitalized patients
Abstract
Background: Antibiotics are essential to effectively treat many hospitalized patients. However, when antibiotics are prescribed incorrectly, they offer little benefit to patients and potentially expose them to risks for complications, including Clostridium difficile infection (CDI) and antibiotic-resistant infections. Information is needed on the frequency of incorrect prescribing in hospitals and how improved prescribing will benefit patients.
Methods: A national administrative database (MarketScan Hospital Drug Database) and CDC's Emerging Infections Program (EIP) data were analyzed to assess the potential for improvement of inpatient antibiotic prescribing. Variability in days of therapy for selected antibiotics reported to the National Healthcare Safety Network (NHSN) antimicrobial use option was computed. The impact of reducing inpatient antibiotic exposure on incidence of CDI was modeled using data from two U.S. hospitals.
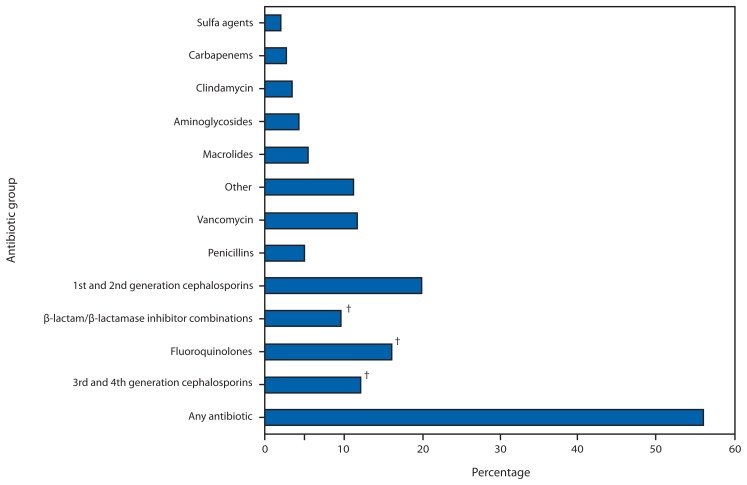
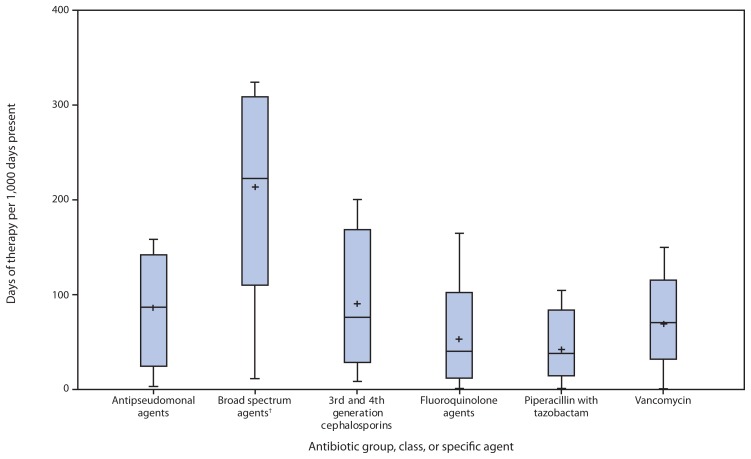
Results: In 2010, 55.7% of patients discharged from 323 hospitals received antibiotics during their hospitalization. EIP reviewed patients' records from 183 hospitals to describe inpatient antibiotic use; antibiotic prescribing potentially could be improved in 37.2% of the most common prescription scenarios reviewed. There were threefold differences in usage rates among 26 medical/surgical wards reporting to NHSN. Models estimate that the total direct and indirect effects from a 30% reduction in use of broad-spectrum antibiotics will result in a 26% reduction in CDI.
Conclusions: Antibiotic prescribing for inpatients is common, and there is ample opportunity to improve use and patient safety by reducing incorrect antibiotic prescribing. Implications for Public Health: Hospital administrators and health-care providers can reduce potential harm and risk for antibiotic resistance by implementing formal programs to improve antibiotic prescribing in hospitals.
Figures
References
-
- Dellit TH, Owens RC, McGowan JE, Jr, et al. Infectious Diseases Society of America; Society for Healthcare Epidemiology of America. Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America guidelines for developing an institutional program to enhance antimicrobial stewardship. Clin Infect Dis. 2007;44:159–77. - PubMed
-
- Hecker MT, Aron DC, Patel NP, Lehmann MK, Donskey CJ. Unnecessary use of antimicrobials in hospitalized patients: current patterns of misuse with an emphasis on the antianaerobic spectrum of activity. Arch Intern Med. 2003;163:972–8. - PubMed
-
- CDC. Antibiotic resistance threats in the United States, 2013. Atlanta, GA: US Department of Health and Human Services, CDC; 2013. Available at http://www.cdc.gov/drugresistance/threat-report-2013.
-
- Costelloe C, Metcalfe C, Lovering A, Mant D, Hay AD. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ. 2010;340:c2096. - PubMed
-
- Lin RY, Nuruzzaman F, Shah SN. Incidence and impact of adverse effects to antibiotics in hospitalized adults with pneumonia. J Hosp Med. 2009;4:E7–15. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
