

Heat waves, aging, and human cardiovascular health
- PMID: 24598696
- PMCID: PMC4155032
- DOI: 10.1249/MSS.0000000000000325
Heat waves, aging, and human cardiovascular health
Abstract
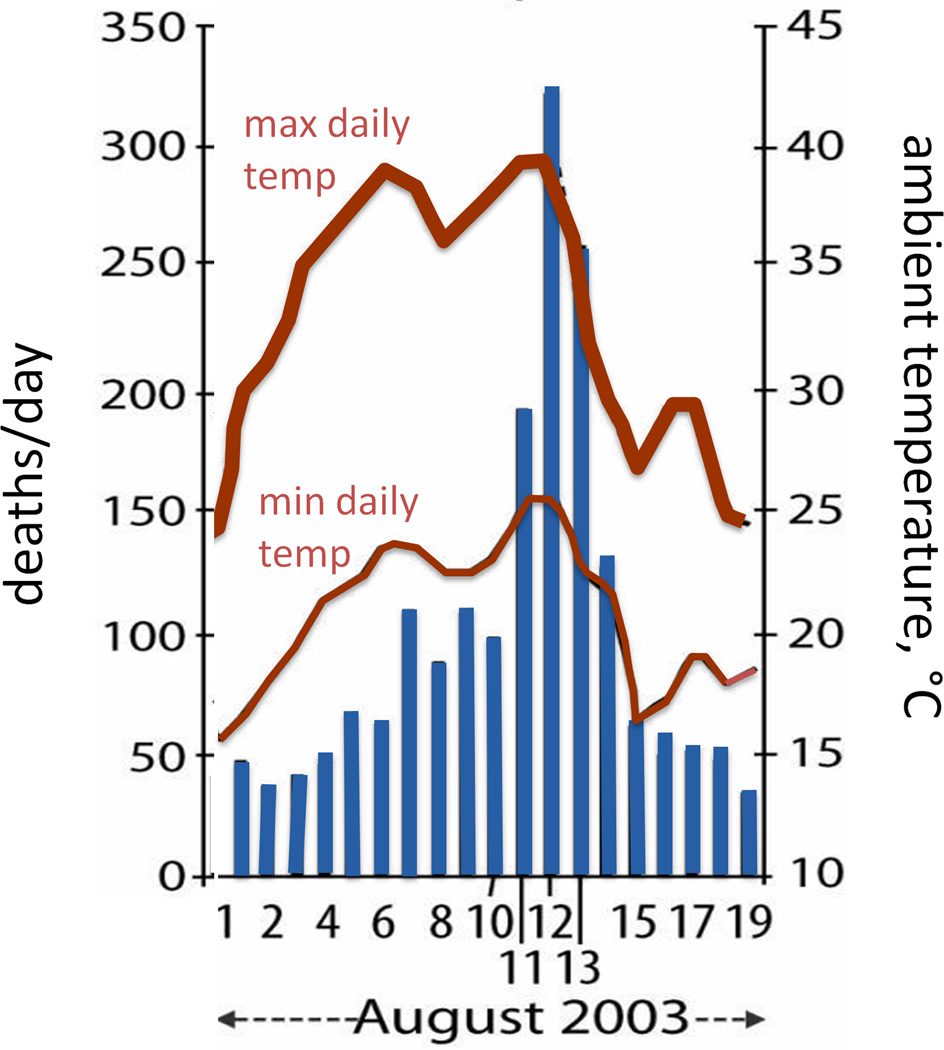
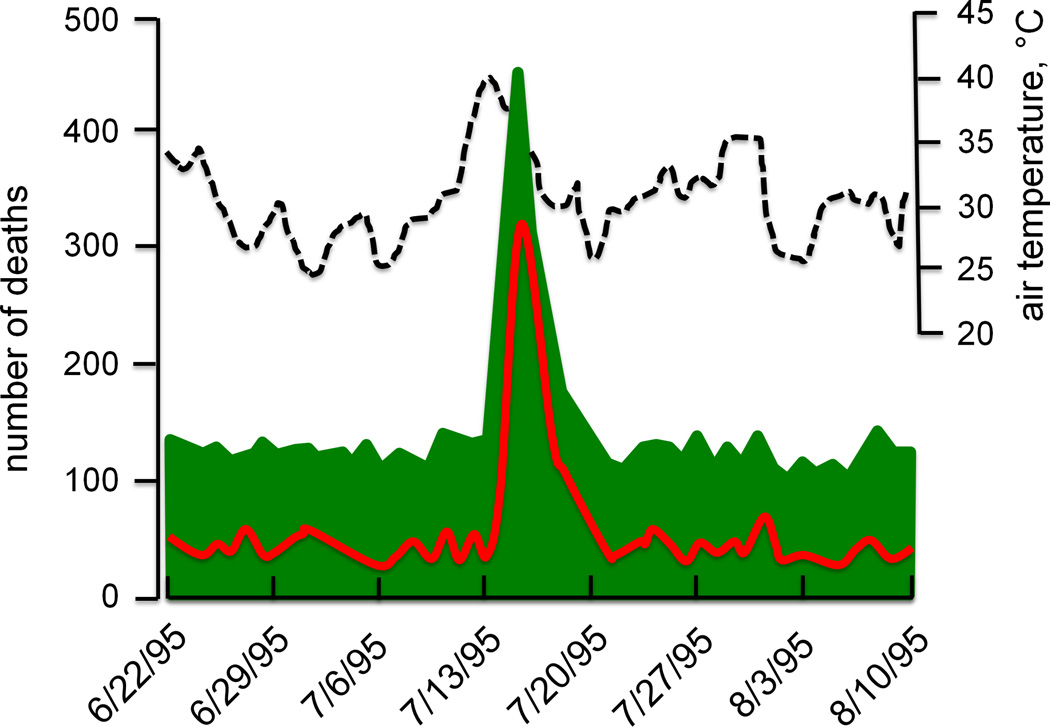
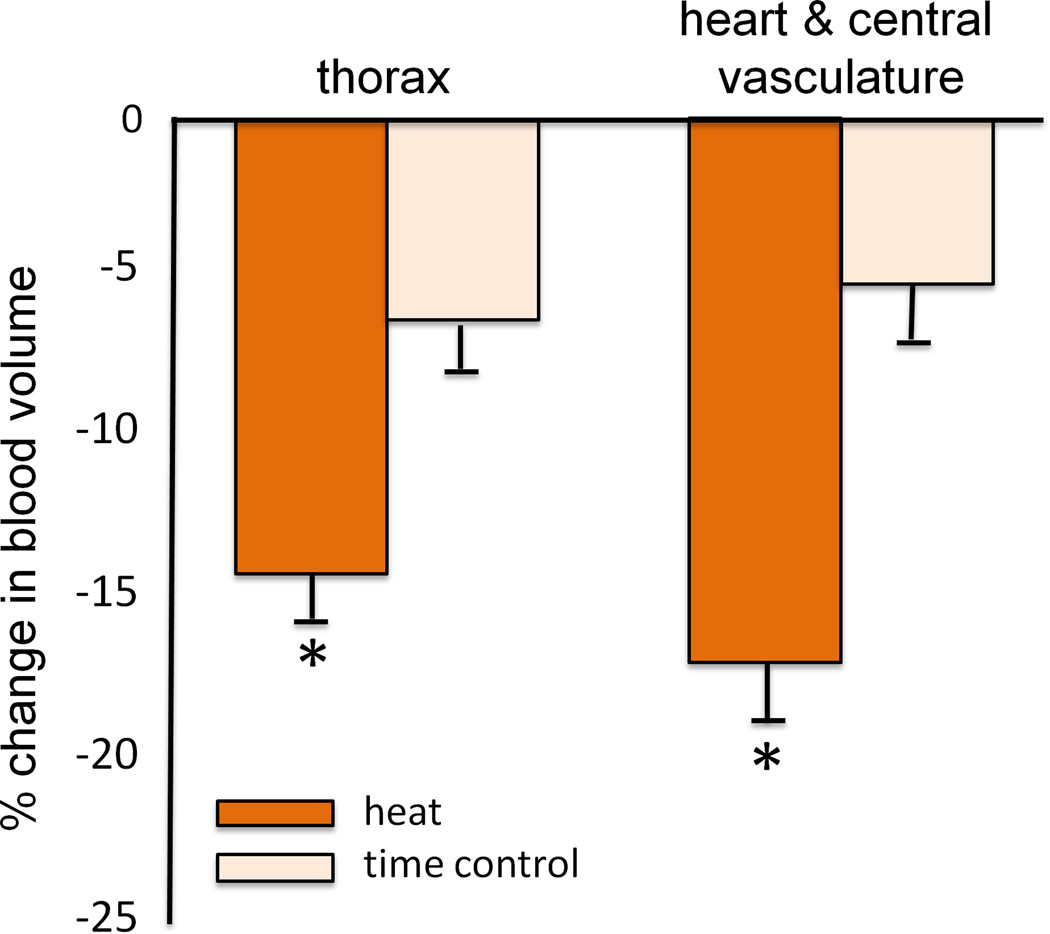
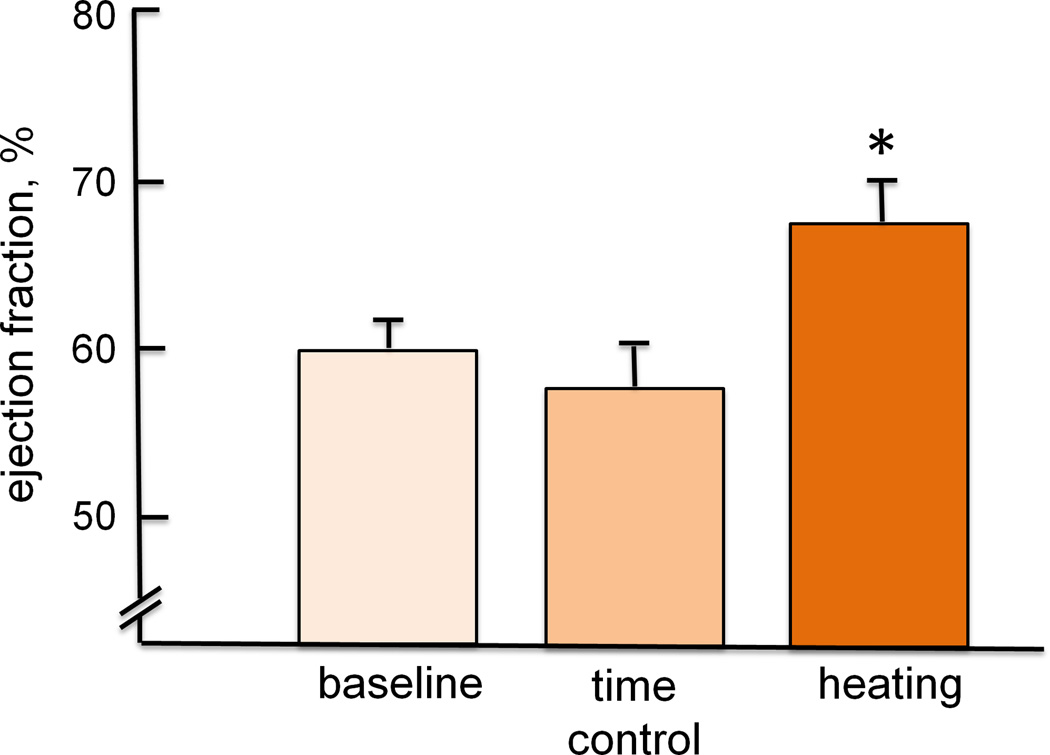
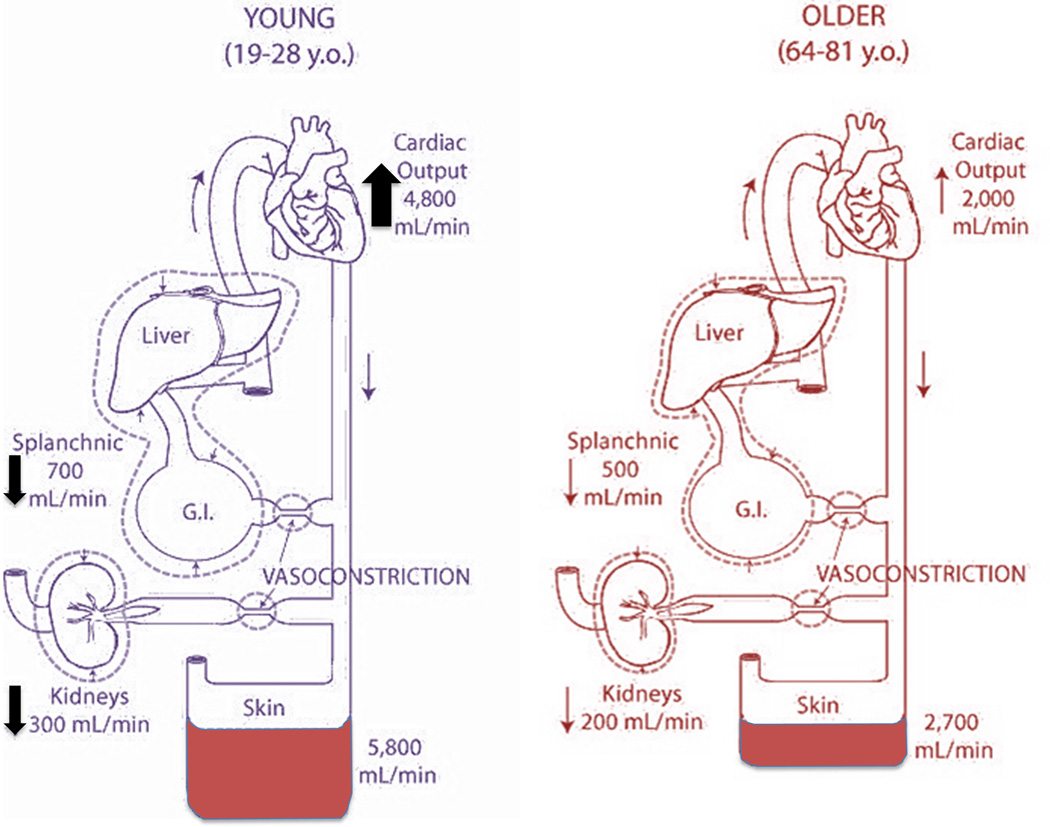
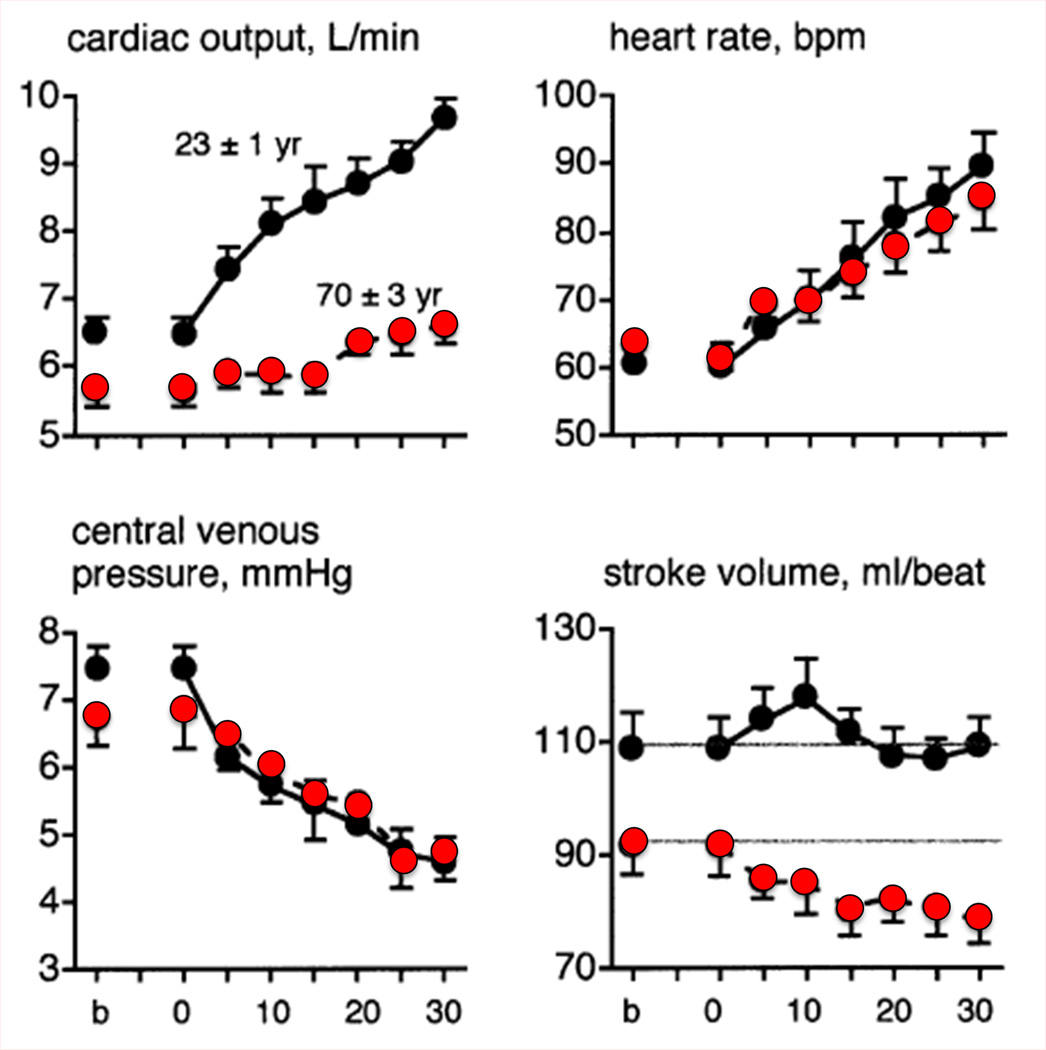
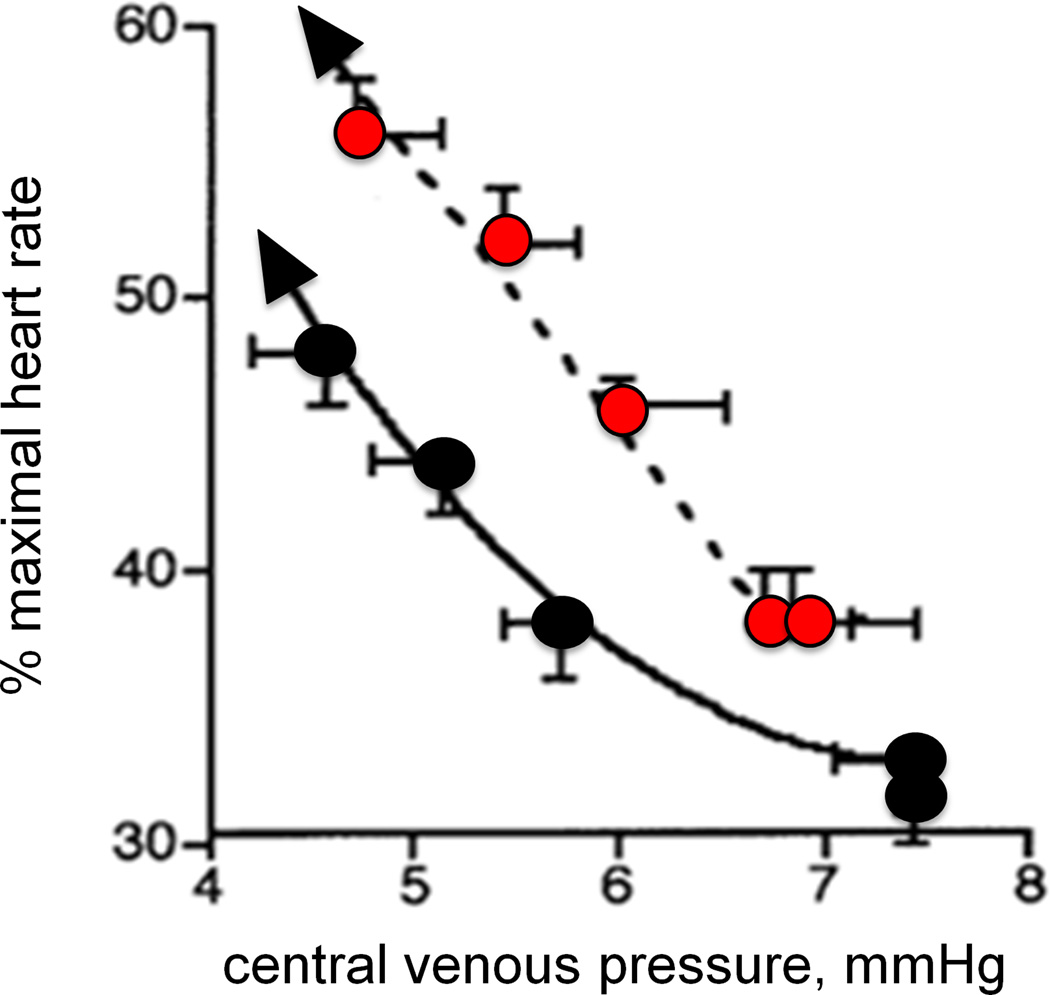
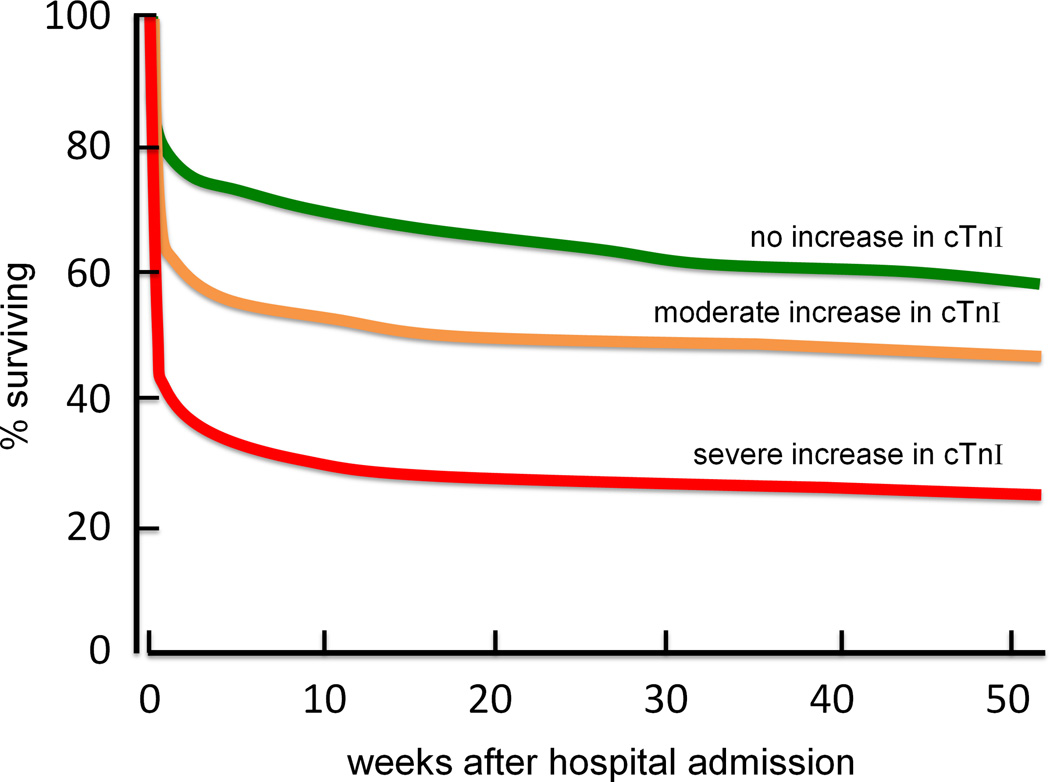
This brief review is based on a President's Lecture presented at the Annual Meeting of the American College of Sports Medicine in 2013. The purpose of this review was to assess the effects of climate change and consequent increases in environmental heat stress on the aging cardiovascular system. The earth's average global temperature is slowly but consistently increasing, and along with mean temperature changes come increases in heat wave frequency and severity. Extreme passive thermal stress resulting from prolonged elevations in ambient temperature and prolonged physical activity in hot environments creates a high demand on the left ventricle to pump blood to the skin to dissipate heat. Even healthy aging is accompanied by altered cardiovascular function, which limits the extent to which older individuals can maintain stroke volume, increase cardiac output, and increase skin blood flow when exposed to environmental extremes. In the elderly, the increased cardiovascular demand during heat waves is often fatal because of increased strain on an already compromised left ventricle. Not surprisingly, excess deaths during heat waves 1) occur predominantly in older individuals and 2) are overwhelmingly cardiovascular in origin. Increasing frequency and severity of heat waves coupled with a rapidly growing at-risk population dramatically increase the extent of future untoward health outcomes.
Conflict of interest statement
The authors have no conflicts of interest to report. No funding was received for this work. The contents of this review do not constitute endorsement by ACSM.
Figures
References
-
- [cited 8/26/2013];A profile of older Americans: 2012. 2012 Available from: http://www.aoa.gov/AoARoot/Aging_Statistics/Profile/2012/2.aspx.
-
- Anderson RK, Kenney WL. Effect of age on heat-activated sweat gland density and flow during exercise in dry heat. Journal of applied physiology. 1987;63(3):1089–1094. - PubMed
-
- Baccini M, Biggeri A, Accetta G, Kosatsky T, Katsouyanni K, Analitis A, et al. Heat effects on mortality in 15 European cities. Epidemiology. 2008;19(5):711–719. - PubMed
-
- Basu R, Malig B. High ambient temperature and mortality in California: exploring the roles of age, disease, and mortality displacement. Environmental research. 2011;111(8):1286–1292. - PubMed
-
- Beckman JS. Oxidative damage and tyrosine nitration from peroxynitrite. Chemical research in toxicology. 1996;9(5):836–844. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
