

Restless legs syndrome status as a predictor for lower physical function
- PMID: 24598708
- PMCID: PMC4001206
- DOI: 10.1212/WNL.0000000000000284
Restless legs syndrome status as a predictor for lower physical function
Abstract
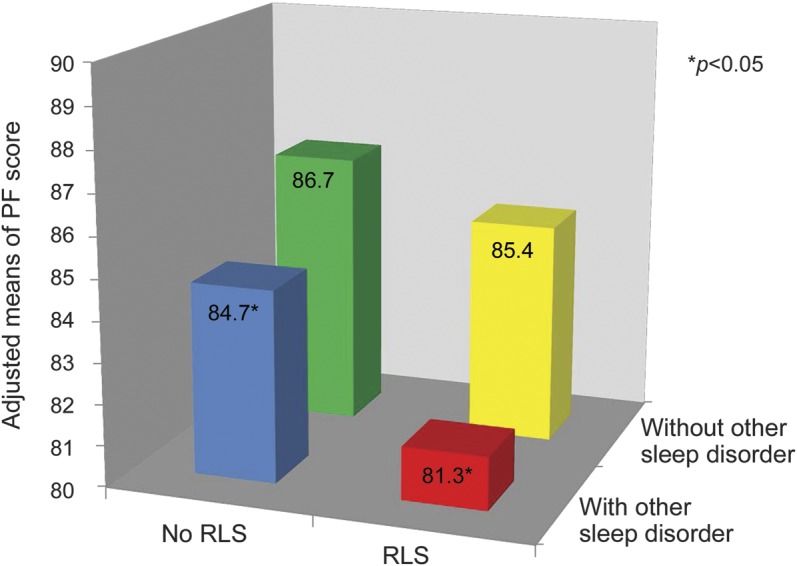
Objective: To examine the potential long-term impact of restless legs syndrome (RLS) and other common sleep complaints on subsequent physical function (PF), we conducted a longitudinal analysis of 12,556 men in the Health Professionals Follow-up Study.
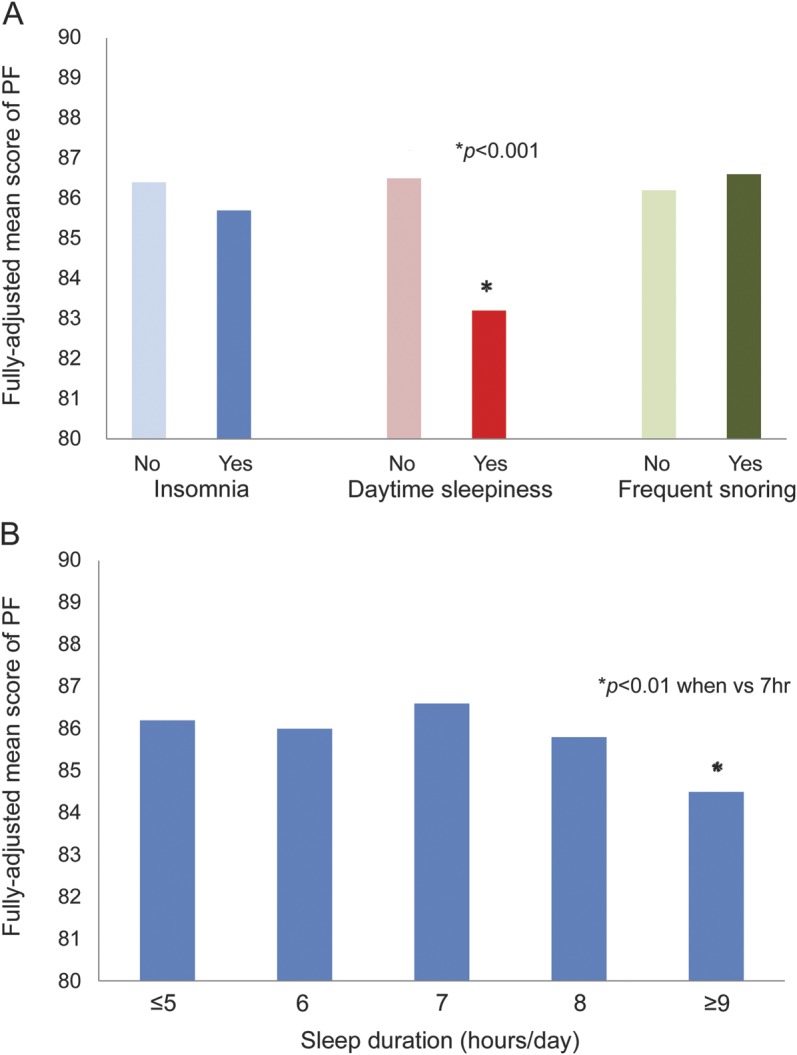
Methods: We used a set of questions recommended by the International RLS Study Group to assess RLS in 2002. We asked questions regarding other sleep complaints--insomnia, sleep fragmentation, and excessive daytime sleepiness--in 2004. We used the Physical Function (PF-10) survey of the Short Form-36 Health Survey to characterize PF in 1996 and 2008. We examined the 2008 PF-10 scores across categories of baseline RLS (2002), adjusted for age, 1996 PF-10 score, and other potential confounders.
Results: The participants with RLS at baseline had significantly lower PF-10 score 6 years later than those without RLS (mean difference = -2.32, p = 0.01), after adjusting for potential confounders. The magnitude of difference in PF-10 score for RLS symptoms ≥ 15 times/month vs no RLS was more than that of a 5-year increase of age or moderate amount of smoking. Having daily daytime sleepiness and sleep duration ≥ 9 hours/day were associated with lower mean PF value than not having these symptoms (p < 0.05 for both).
Conclusions: RLS and other sleep complaints are associated with lower PF. Our findings need to be replicated by more longitudinal studies including women and populations of other social and cultural backgrounds. It is important to understand whether RLS is an independent risk factor or a marker for other unknown risk factors for disability.
Figures
Comment in
-
Restless legs syndrome: a predictor of lower physical function.Neurology. 2014 Apr 8;82(14):1198-9. doi: 10.1212/WNL.0000000000000298. Epub 2014 Mar 5. Neurology. 2014. PMID: 24598710
References
-
- Broman JE, Mallon L, Hetta J. Restless legs syndrome and its relationship with insomnia symptoms and daytime distress: epidemiological survey in Sweden. Psychiatry Clin Neurosci 2008;62:472–475 - PubMed
-
- Earley CJ, Silber MH. Restless legs syndrome: understanding its consequences and the need for better treatment. Sleep Med 2010;11:807–815 - PubMed
-
- Trenkwalder C, Hogl B, Winkelmann J. Recent advances in the diagnosis, genetics and treatment of restless legs syndrome. J Neurol 2009;256:539–553 - PubMed
-
- Abetz L, Allen R, Follet A, et al. Evaluating the quality of life of patients with restless legs syndrome. Clin Ther 2004;26:925–935 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical