

Effects of beta-blockers on heart failure with preserved ejection fraction: a meta-analysis
- PMID: 24599093
- PMCID: PMC3944014
- DOI: 10.1371/journal.pone.0090555
Effects of beta-blockers on heart failure with preserved ejection fraction: a meta-analysis
Abstract
Background: Effects of beta-blockers on the prognosis of the heart failure patients with preserved ejection fraction (HFpEF) remain controversial. The aim of this meta-analysis was to determine the impact of beta-blockers on mortality and hospitalization in the patients with HFpEF.
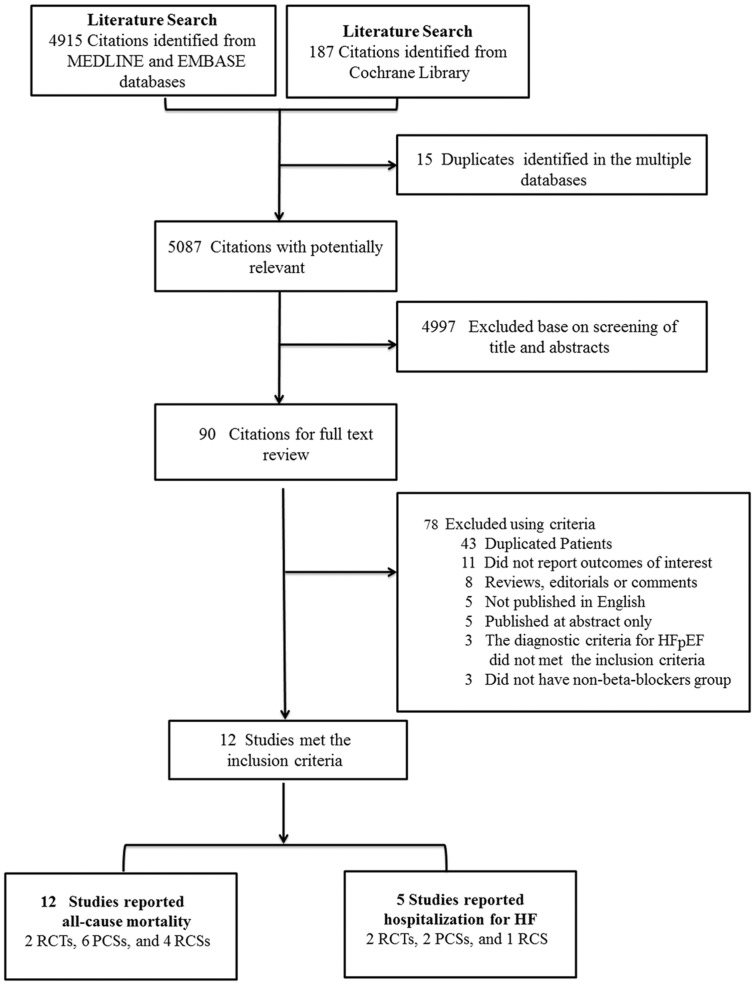
Methods: A search of MEDLINE, EMBASE, and the Cochrane Library databases from 2005 to June 2013 was conducted. Clinical studies reporting outcomes of mortality and/or hospitalization for patients with HFpEF (EF ≥ 40%), being assigned to beta-blockers treatment and non-beta-blockers control group were included.
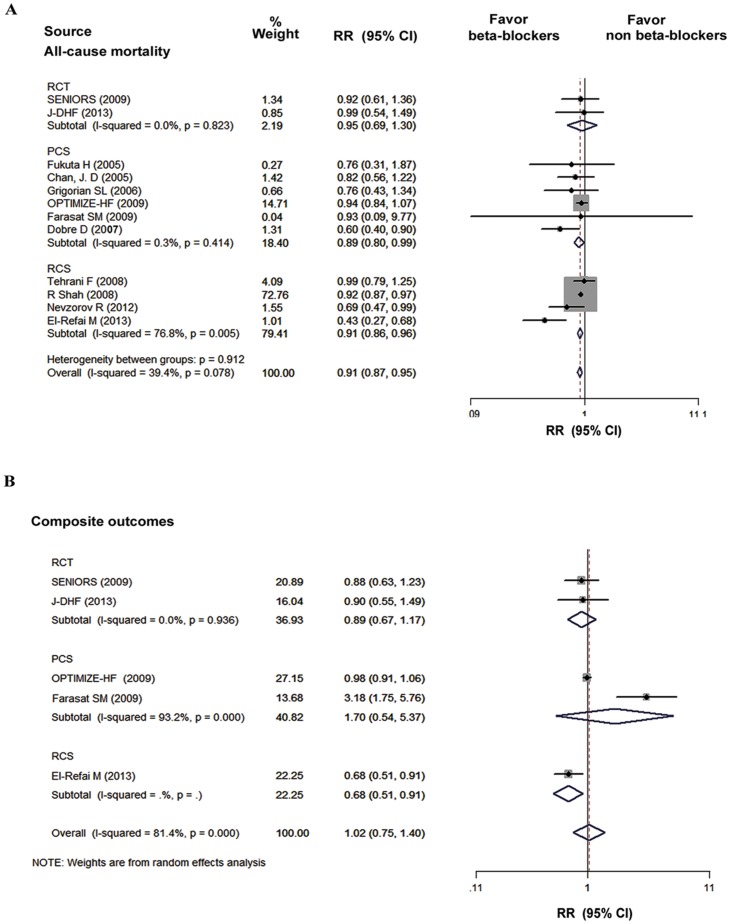
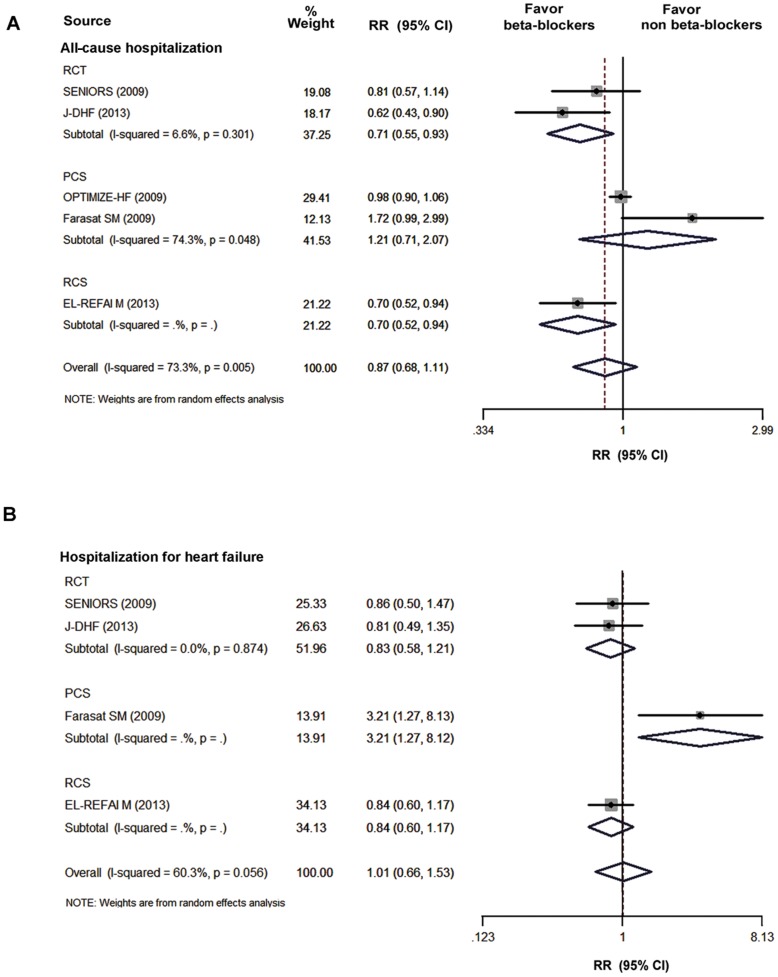
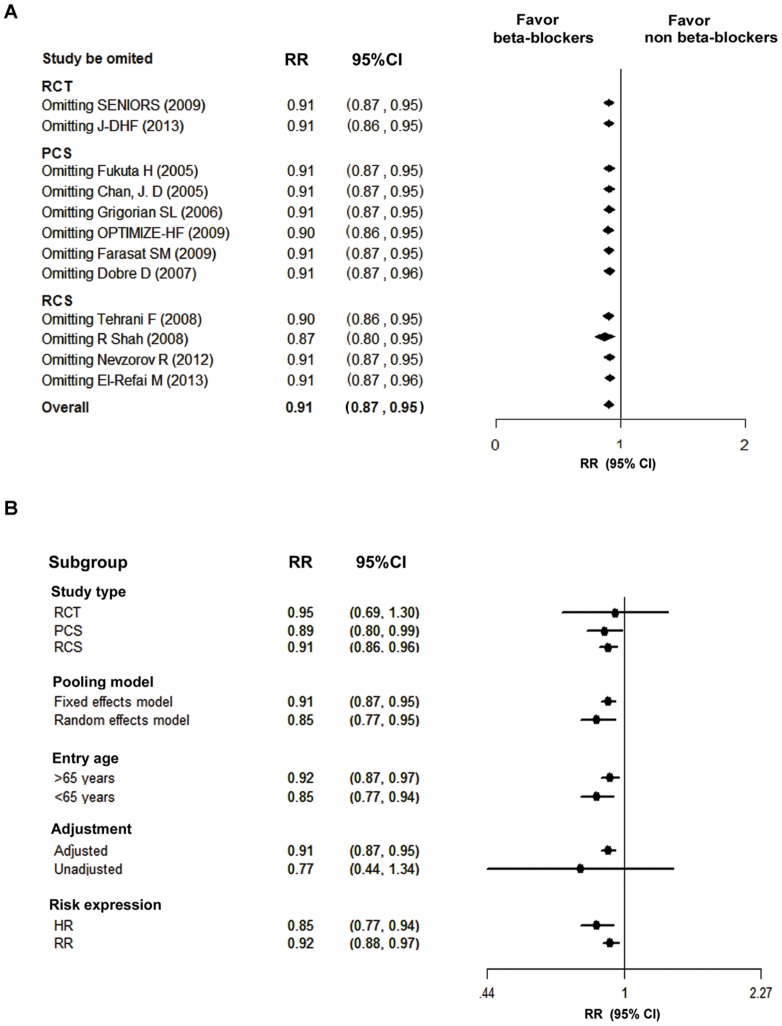
Results: A total of 12 clinical studies (2 randomized controlled trials and 10 observational studies) involving 21,206 HFpEF patients were included for this meta-analysis. The pooled analysis demonstrated that beta-blocker exposure was associated with a 9% reduction in relative risk for all-cause mortality in patients with HFpEF (95% CI: 0.87 - 0.95; P < 0.001). Whereas, the all-cause hospitalization, HF hospitalization and composite outcomes (mortality and hospitalization) were not affected by this treatment (P=0.26, P=0.97, and P=0.88 respectively).
Conclusions: The beta-blockers treatment for the patients with HFpEF was associated with a lower risk of all-cause mortality, but not with a lower risk of hospitalization. These finding were mainly obtained from observational studies, and further investigations are needed to make an assertion.
Conflict of interest statement
Figures
References
-
- Masoudi FA, Havranek EP, Smith G, Fish RH, Steiner JF, et al. (2003) Gender, age, and heart failure with preserved left ventricular systolic function. J Am Coll Cardiol 41: 217–223. - PubMed
-
- Smith GL, Masoudi FA, Vaccarino V, Radford MJ, Krumholz HM (2003) Outcomes in heart failure patients with preserved ejection fraction: mortality, readmission, and functional decline. J Am Coll Cardiol 41: 1510–1518. - PubMed
-
- Packer M, Coats AJ, Fowler MB, Katus HA, Krum H, et al. (2001) Effect of carvedilol on survival in severe chronic heart failure. N Engl J Med 344: 1651–1658. - PubMed
-
- Krum H, Roecker EB, Mohacsi P, Rouleau JL, Tendera M, et al. (2003) Effects of initiating carvedilol in patients with severe chronic heart failure: results from the COPERNICUS Study. JAMA 289: 712–718. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
