

Obesity, hypertension, and chronic kidney disease
- PMID: 24600241
- PMCID: PMC3933708
- DOI: 10.2147/IJNRD.S39739
Obesity, hypertension, and chronic kidney disease
Abstract
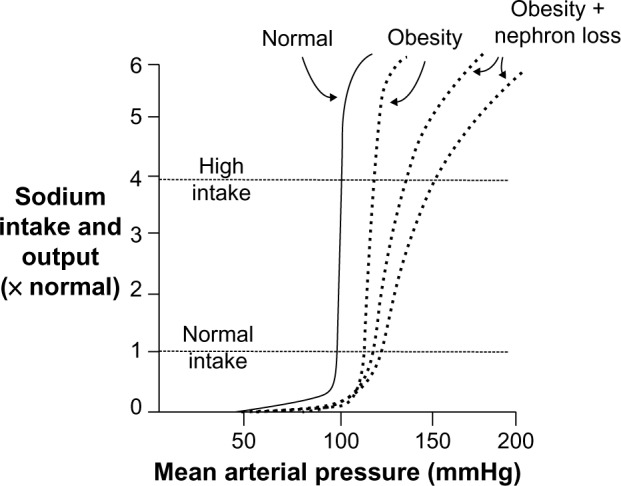
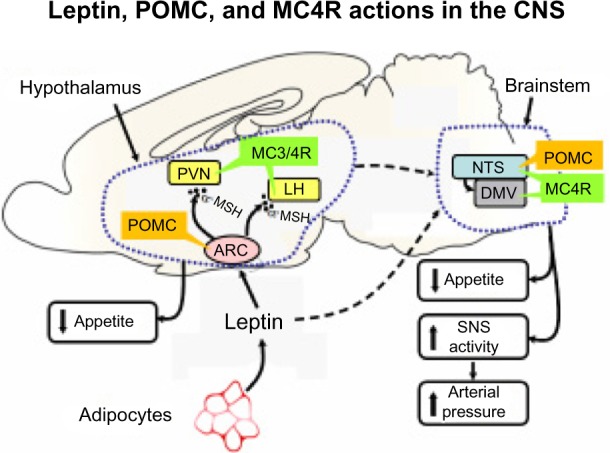
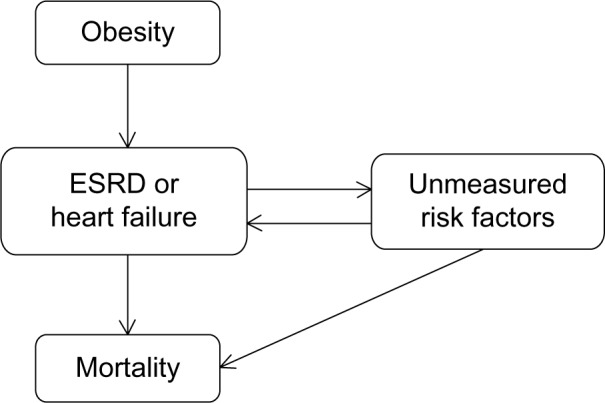
Obesity is a major risk factor for essential hypertension, diabetes, and other comorbid conditions that contribute to development of chronic kidney disease. Obesity raises blood pressure by increasing renal tubular sodium reabsorption, impairing pressure natriuresis, and causing volume expansion via activation of the sympathetic nervous system and renin-angiotensin-aldosterone system and by physical compression of the kidneys, especially when there is increased visceral adiposity. Other factors such as inflammation, oxidative stress, and lipotoxicity may also contribute to obesity-mediated hypertension and renal dysfunction. Initially, obesity causes renal vasodilation and glomerular hyperfiltration, which act as compensatory mechanisms to maintain sodium balance despite increased tubular reabsorption. However, these compensations, along with increased arterial pressure and metabolic abnormalities, may ultimately lead to glomerular injury and initiate a slowly developing vicious cycle that exacerbates hypertension and worsens renal injury. Body weight reduction, via caloric restriction and increased physical activity, is an important first step for management of obesity, hypertension, and chronic kidney disease. However, this strategy may not be effective in producing long-term weight loss or in preventing cardiorenal and metabolic consequences in many obese patients. The majority of obese patients require medical therapy for obesity-associated hypertension, metabolic disorders, and renal disease, and morbidly obese patients may require surgical interventions to produce sustained weight loss.
Keywords: glomerular filtration rate; renin–angiotensin–aldosterone system; sodium reabsorption; sympathetic nervous system; type II diabetes; visceral adiposity.
Figures





References
-
- Fact Sheet N°311 [webpage on the Internet] Geneva: World Health Organization; [Accessed October 18, 2013]. Obesity and overweight. [updated Mar 2013; cited October 24, 2013]. Available from: http://www.who.int/mediacentre/factsheets/fs311/en/index.html.
-
- Adult obesity facts [webpage on the Internet] Atlanta: Center for Disease Control and Prevention; [Accessed on September 14, 2013]. Obesity and overweight trends in the US, 2011. [updated Aug 2013; cited October 24, 2013]. Available from: http://www.cdc.gov/nccdphp/dnpa/obesity/trend/index.htm.
-
- Hall JE, Henegar JR, Dwyer TM, et al. Is obesity a major cause of chronic renal disease? Adv Ren Replace Ther. 2004;11(1):41–54. - PubMed
-
- Tchernof A, Després JP. Pathophysiology of human visceral obesity: an update. Physiol Rev. 2013;93(1):359–404. - PubMed
-
- Hall JE, Crook ED, Jones DW, Wofford MR, Dubbert PM. Mechanisms of obesity-associated cardiovascular and renal disease. Am J Med Sci. 2002;324(3):127–137. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
