

Pharyngeal airway space, hyoid bone position, and head posture after bimaxillary orthognathic surgery in Class III patients: long-term evaluation
- PMID: 24601894
- PMCID: PMC8641282
- DOI: 10.2319/072213-534.1
Pharyngeal airway space, hyoid bone position, and head posture after bimaxillary orthognathic surgery in Class III patients: long-term evaluation
Abstract
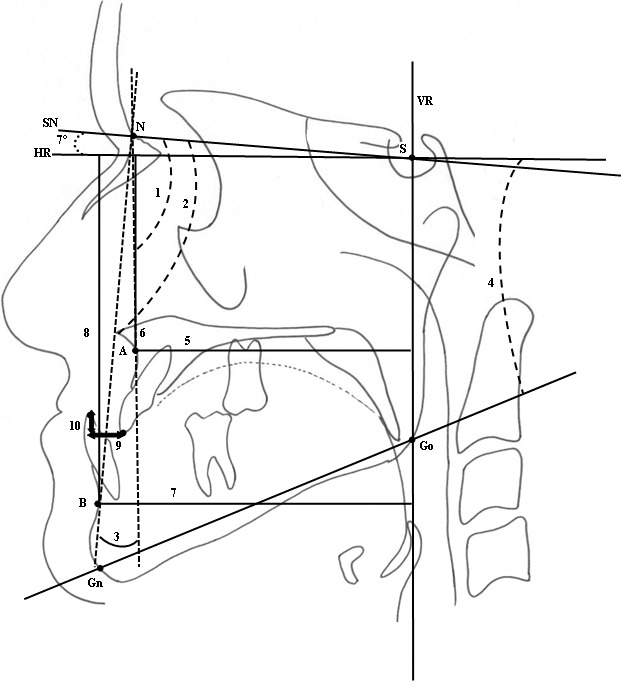
Objective: (1) To determine the effect of bimaxillary orthognathic surgery on pharyngeal airway, hyoid bone, and craniocervical posture in Class III bimaxillary surgery patients. (2) To evaluate short-term and long-term results. (3) To compare short- and long-term values.
Materials and methods: Twenty-six Class III adult patients treated with bimaxillary surgery were included in the study. Cephalometric records were taken before treatment (T1), before surgery (T2), and 5 months (T3), 1.4 years (T4), 3 years (T5), and 5 years (T6) postsurgery.
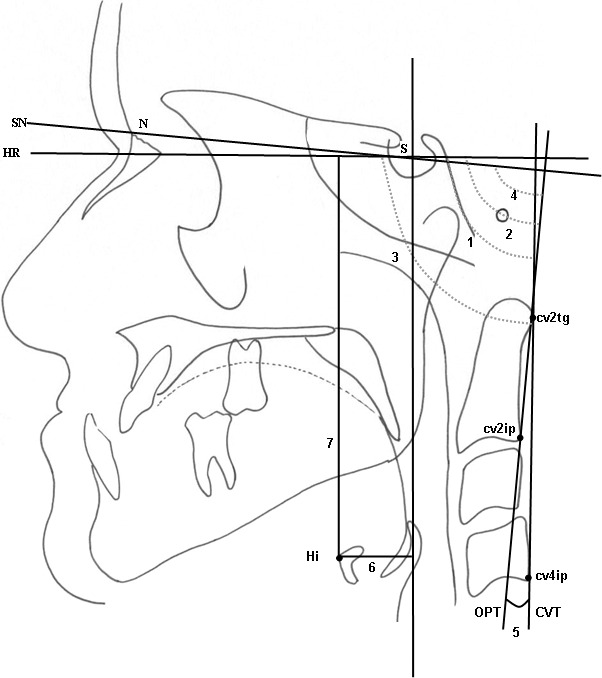
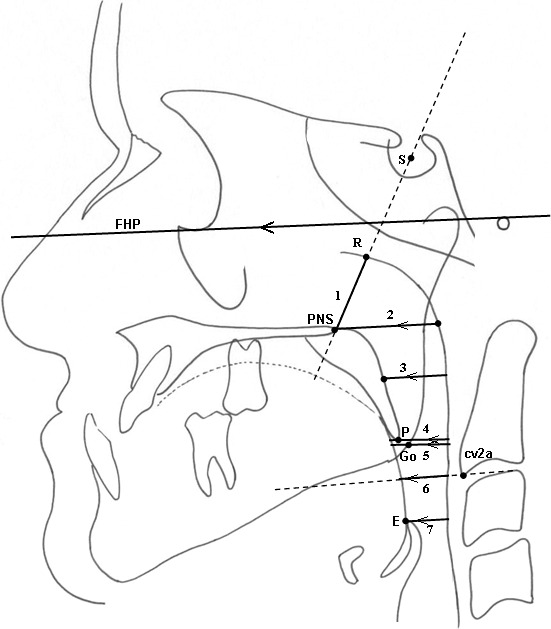
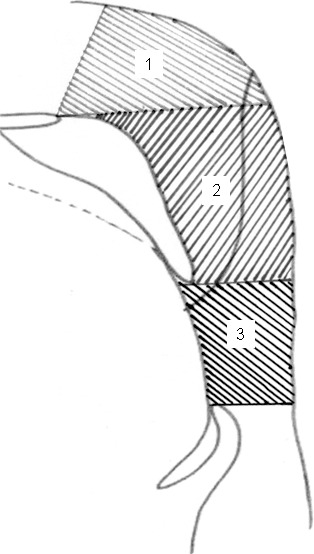
Results: No significant differences were identified in craniocervical angulation between time intervals. There was a significant superior movement of hyoid bone at postsurgery (T3; P < .05); however, adaptation occurred to the normal position in the long term. A nonsignificant decrease occurred at the oropharyngeal middle pharyngeal distance parameter; however, this was compensated with a significant increase between T5 and T6 (P < .001). A significant decrease was observed in the hypopharyngeal Go-P parameter between T3 and T1 (P < .01), but it recovered with a nonsignificant increase in the long term. A significant increase in nasopharyngeal area was observed between T3 and T1 (P < .05). The hypopharyngeal area significantly increased between T5 and T6, and PNS-R significantly increased between T3 and T1 (P < .05).
Conclusion: The pharyngeal areas adversely affected after surgery recover at long-term follow-up; thus, adaptation occurs after bimaxillary surgery.
Keywords: Airway; Bimaxillary surgery; Class III; Long-term.
Figures
References
-
- Hochban W, Schurmann R, Bradenburg U, Conradt R. Mandibular setback for the surgical correction of mandibular hyperplasia—does it provoke sleep-related breathing disorders. Int J Oral Maxillofac Surg. 1996;25:333–338. - PubMed
-
- Güven O, Saraçoğlu U. Changes in pharyngeal airway space and hyoid bone positions after body ostectomies and sagittal split ramus osteotomies. J Craniofac Surg. 2005;16:23–30. - PubMed
-
- Enacar A, Aksoy AU, Sençift Y, Haydar B, Aras K. Changes in hypopharyngeal airway space and in tongue and hyoid bone positions following the surgical correction of mandibular prognathism. Int J Adult Orthodon Orthognath Surg. 1994;9:285–290. - PubMed
-
- Achilleos S, Krogstad O, Lyberg T. Surgical mandible setback and changes in uvuloglossopharyngeal morphology and head posture: a short- and long-term cephalometric study in males. Eur J Orthod. 2000;22:383–394. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
